
Time-Restricted Eating or Intermittent Fasting Linked to 91% Higher Deaths
May 05 2024
This recent paper was all over the media, showing that time-restricted eating was linked with a shocking 91% increase in heart disease-related deaths.
What is time-restricted eating?
It is a form of intermittent fasting where you restrict your food intake to a short time frame during the day, say 8 hours or less, and fast for the remaining hours.

What did the study show?
Briefly, the study involved 20,000 US adults providing data on what they ate, and at what times, over a 24-hour period on two separate occasions from 2003 to 2018. The study was a poster for the American Heart Association’s Epidemiology of Prevention conference in Chicago in March 2024. So the paper hasn’t gone through peer review.
Increase in Deaths: People who restricted eating to less than 8 hours per day were associated with a 91% greater number of deaths due to heart-related diseases compared to folks who followed a traditional pattern of eating their food across 12 to 16 hours each day.
What does 91% increase in deaths mean?
The only reason this was picked by media is due to the large increase in mortality of 91%. But isn’t 91% a huge increase in deaths???
- Relative Risk (IRR): The risk here is presented in relative terms. It means the risk is almost 100% greater than/relative to the control group, which sounds huge. Relative risk always tends to exaggerate the risk more than what it actually is.
- Absolute Risk (AR): The best way to communicate risk is using absolute risk. Here the absolute risk difference (unadjusted) is 3.9% or 4%, which means out of 100 people, TRE is linked to 4 more deaths in 8 years. It clearly doesn’t sound so shocking, right? And if the results were expressed in AR, this study would have never made the headlines.
- AR vs RR example: If there was 1 death in the control group out of 100 and just 2 deaths in the diet group of 100, the relative risk (dividing risk in diet grp. by control grp) is 2.0, which represents a 100% increase in deaths. The absolute risk difference is 1% (calculated by subtracting control risk from diet grp. risk). So a 100% increase in deaths was actually just one more death compared to the control group!

So many experts in so many news articles and Twitter commented about reverse causation, confounding, low sample sizes, and self-reporting of dietary habits, problems with observational studies, but not even a single person ever bothered to express risk in absolute terms. Hence the reason for this short, but important post.
Conclusions
- Time-restricted eating was ‘associated’ with a 4% increase or simply 4 more deaths in 8 years.
- Next time you hear about ‘impressive’ changes in risk, ask for absolute changes.
Related Articles


My Thoughts on the Controversial Cochrane Mask Study
May 01 2023
Community masking was one of the most hotly debated topics during the pandemic. And the recent Cochrane study made the topic even more controversial by questioning the efficacy of masks. Here follows my take on this critical study:
What did they do?
Cochrane is a non-profit organization that conducts systematic reviews on healthcare topics. A Systematic review summarizes a collection of studies on a particular topic and thus shows the totality of the evidence. And Cochrane reviews are considered the gold standard due to their rigorous methodology.
The first mask review was published in 2001, and it has been updated in 2009, 2020, and now in 2023 (1). In 2020, the authors decided to only include randomized controlled trials instead of observational studies, which led to the inclusion of two studies that took place during the pandemic.
The questions they asked:
- Can surgical/medical masks prevent the spread of respiratory virus infections and lab-confirmed infections?
- Can N95 masks prevent the spread of respiratory virus infections compared to medical/surgical masks?
- Can hand hygiene (hand washing & sanitizer use) prevent the spread of respiratory virus infections?
So what did they find out about masks?
- Viral respiratory illness: For surgical masks, the study concluded “Wearing masks in the community probably makes little or no difference to the outcome of influenza‐like illness/COVID‐19 like illness compared to not wearing masks risk ratio (RR) 0.95, 95% confidence interval (CI) 0.84 to 1.09; 9 trials, 276,917 participants; moderate‐certainty evidence”
- Laboratory‐confirmed viral respiratory illness- Similarly, for lab confirmed outcomes showed similar results that masks probably makes little or no difference.
I have highlighted two words “probably” and “little or no difference” since these are the key words that say everything. I have omitted N95 masks and hand hygiene questions for the sake of brevity.
What do the results really mean?
Several articles from major news outlets and experts have commented on the review, but few have interpreted it correctly. It is important to note that Cochrane uses a specific methodology called GRADE to summarize and communicate the results. And without having a decent understanding of GRADE, the results can be very confusing.
GRADE mainly uses two concepts to summarize study findings.
1. Size of the difference
2. Certainty rating
- Little to no difference: The size of the difference here of 0.95 is considered to be trivial by the authors hence the use of “little to no difference”. But what the heck does 0.95 mean? I have yet to see anyone who interpreted these numbers properly
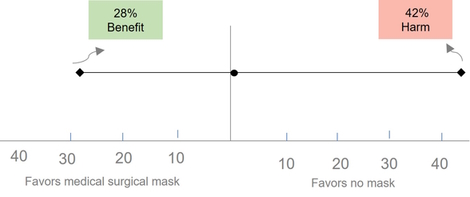
- 0.95: A risk of 0.95 means a 5% reduction in infections. However, this does not mean that 5 out of 100 people will benefit. Rather, if 1000 people wore masks, 8 fewer people would be infected or would receive a benefit.
- Confidence interval (CI): The confidence interval (CI) of 0.84 to 1.09 shows us the precision or uncertainty in the results. This means that the 5% estimate could range from as low as 26 fewer people being infected to 14 more people getting infected (out of 1000).
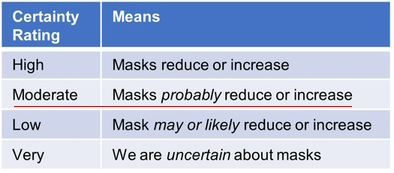
- Moderate certainty means? But how certain or confident are we about this estimate of 5% reduction? That’s where the GRADE certainty ratings come in. As shown below, there are 4 certainty criteria (High, Moderate, Low, & Very low) which communicates different degrees of confidence in the results. Every review starts out at high certainty and get downgraded based on how well the study was conducted based on 4 domains.
Here the certainty rating was downgraded from high to moderate because of high risk of bias (or poor study quality) for viral illness and for the lab‐confirmed influenza/SARS‐CoV‐2 for imprecision. Thus, combining the magnitude of benefit and the certainty rating, the authors end up with the statement of masking “probably” has “little to no difference”.
Bear in mind that a rating of high certainty reviews is usually seen for drug trials and the majority of the Cochrane reviews end up being low or very low certainty. A moderate certainty for behavioral intervention is pretty good and pretty damning evidence against wearing masks. This is why the lead author of the study in another article wrote, “There is just no evidence that they make any difference. Full stop.”
So should you stop wearing masks?
My thoughts:
It is important to note that the GRADE approach requires judgement and could vary between individuals. What it lacks in objectivity is supposedly made up in transparency, i.e, how authors came to their decisions. Below I show some alternative conclusions that are equally correct within the GRADE approach:
Viral respiratory illness
- Mask may reduce viral infections: Since the authors haven’t transparently stated what is trivial or an important reduction, they could have very well concluded that surgical masks may show an effect based on the 5% reduction. And since the interval captures both benefit (16%) and harm (9%), they could downgrade it for imprecision and end up with a “Low” certainty than moderate certainty. This conclusion makes more sense since we don’t know what is trivial or a small, important effect is, but we know there is some non-zero (5%) effect/reduction.
- Is 5% trivial: A good question is 5% a small, but important or trivial benefit ? While a reduction of 5% or 8 fewer people out of 1000 may seem trivial from an individual perspective, it could have a significant impact from a population or public health standpoint, especially for a highly contagious serious infection like COVID-19. It’s important to remember that mask mandates were not just meant to prevent infection in the wearer, but also to prevent the spread of infection to others. This is totally different from our typical diseases, like heart disease. You don’t transmit heart disease or diabetes, do you? To put these numbers in perspective, the Pfizer COVID vaccine showed an absolute reduction of 0.7% (7 fewer people out of 1000), but we know that number could quickly escalate to 500 out of 1000, if left unvaccinated. Statins, the number one selling drugs, show 10 fewer deaths and 13 fewer heart attacks in 1000 people taking them for 4-5 years (3). The bottom line is that the authors could have concluded that there may be an effect/reduction and let the readers decide for themselves if this effect is important or trivial.
Lab-confirmed viral illness
- Risk of bias: The authors downgraded the certainty rating for risk of bias for the outcome of viral illness. However, they did not downgrade for lab-confirmed outcome and haven’t transparently justified it either. All the studies are clearly of “high risk” of bias as shown by the red circle. The 3 studies contributing the most weight (A,B,C) is also at high risk.
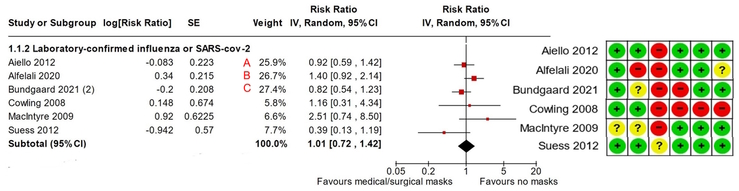
- Precision : Several folks have argued that the confidence interval (CI) for lab confirmed outcome is quite wide (0.72 to 1.42), representing a 28% decrease to a 42% increase, and therefore the results should be considered uncertain. This uncertainty is related to the threshold that the authors consider to be trivial or important, which they have not explicitly stated in the article. Interestingly, the authors concluded that hand hygiene “may reduce infection” with a 14% reduction (0.86). If a 14% reduction is good, then a 28% to 42% change from masking would certainly show large benefit and harm (42% is 3 times 14%!), right? This would mean that the certainty rating should be downgraded by 2 or 3 levels, and not just by one, indicating low or very low certainty about the benefits of masking. Even without GRADE guiding us, it makes a lot of common sense to say that we are uncertain, since the true effect is equally compatible with a large benefit and harm. This is what GRADE recommends as well, as shown below in their latest paper on precision. (2)
“Using the CI approach, when the CI is wide and considerably cross the
threshold(s) of interests (i.e., one or both boundaries of Cls suggest
inferences appreciably different from point estimate), one should consider
rating down two levels for imprecision, and when the Cl is very wide that the
two boundaries of Cl suggest very different inferences, one should consider
rating down three levels for imprecision.”
So, considering the serious risk of bias and imprecision, the lab confirmed outcome could have easily ended up to be “very uncertain”. Or in other words, we could say are very uncertain about masks.
A few other criticisms:
- Low adherence: Some folks have argued that since the authors reported low adherence t0 mask wearing, the conclusions are not very credible. But this is exactly how real life works. If you ask people to wear masks, some will, some will not, and many will wear them improperly. It is called the “Intention to treat” approach, which has been the standard approach for analyzing trials for over 100 years!
- Promote mask wearing vs. mask wearing: The Cochrane editor and a few others have argued that the review is about “promoting” mask wearing rather than wearing masks. While this is true, it’s also true for most behavioral interventions, like physical activity, nutrition, drugs and so forth. Therefore, if we adopt this argument, it follows that we should update all reviews along similar lines.
Decision making: On a final note, decisions about wearing masks, or any interventions for that matter, are not just about looking at the benefits. Instead, decision making involves weighing the benefit, risk, and burden, which in turn depends on the values and preferences of the individual. For example, a trivial benefit for one person could be an important benefit for another, which explains a lot of the polarized opinions on this topic.
Conclusions:
In summary, instead of concluding masks probably don’t work, conclusions for this review could have ranged from “wearing masks in the community may reduce infections” to “we are very uncertain of the effects of mask wearing on infections”. This also means we need better quality studies and more of them.
So, don’t throw away your masks!
Related Articles






Is This The Magic Weight Loss Pill?
August 08 2022
There has been number of weight loss drugs in the market. But this one has surprised a lot of obesity experts - in a good way.

Around 40% of the US adults are obese and these numbers are steadily getting worse. The study in question was recently published in NEJM - one of the premier medical journals. So let’s take a closer look:
So what was the study design?
- Population: 1960 participants greater than BMI of 30 (obese) or 27 or greater with one or more treated or untreated risk factors from 129 sites in 16 countries. So an international multi-center trial.
- Intervention: The intervention group took once a week injection Semaglutide (at a dose of 2.4 mg) plus lifestyle changes (diet and exercise)
- Control: The control group took a placebo injection plus life style intervention.
- Outcomes: The primary outcome was the % of weight lost.
What were the results?
The mean BMI was around 37 (Class 2 obesity). After 68 weeks, the drug group lost 15% while the placebo lost 2% of their body weight. That is, the drug group lost 15.3 kg while the placebo group lost a meagre 2.6kg. So almost a 13 kg weight loss! For the metrically impaired, that is a whopping 30 lbs!
My comments:
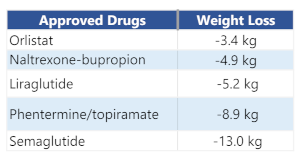
Weight loss: Currently available FDA approved obesity drugs have struggled to show double-digit (>10%) weight loss and shows 5-8% weight loss. At present, the most efficacious drug (Phentermine/topiramate) reduces bodyweight by 8% compared to placebo. In contrast, the avg weight loss in this study was a remarkable 15%. Further, 1/3rd of the participants showed a 20% weight reduction which is close to results for bariatric surgery (around 25% using sleeve gastrectomy)! Rightfully so, these results have pleasantly surprised a lot of the obesity experts.
1-yr Weight change compared to placebo for FDA approved drugs
Mechanism: So how does it work? It works by mimicking a hormone that is produced in the body after you eat. The hormone suppresses appetite/food intake by acting on appetite centers in your brain. So the drug is essentially rewiring your brain. Partcipants in the study reported less appetite and food cravings, better control of eating and lower relative preference for fatty, energy-dense foods. Mind you, most obesity drugs work their “magic” by suppressing appetite and thus making you eat less!
Harms: Nausea and diarrhea were the major complaints. Other events were constipation, nausea, abdominal pain, headache, or fatigue. For the forgetful, let’s not forget the checkered history of weight loss drugs: To name a few recent ones, Sibutramine was withdrawn in 2010 due to increase in heart attacks, strokes, and deaths; Lorcaserin in 2020 due to increase in cancers. In other words, harms of the drugs are as important as weight loss benfits. Long-term side effects of the drug are still unknown, especially important when dealing with chornic conditions like obesity.
Cost: I like everything about the drug, except the horrible price: Slightly more than thousand dollars for a month’s supply. And guess what, insurance do not cover weight loss drugs either. They still argue that obesity is a behavioral choice and not a disease. Several smart folks have argued obesity to be best considered as a chronic condition requiring lifelong medications just like every other health conditions, like heart disease and diabetes.
Other studies: This study was the first of the STEP 1 Trials. They have concluded around 8 studies (STEP 1-8) looking at different populations and dosages and cardiovascular outcomes. For example, in people with diabetes and in east Asians. All seem to show similar and positive effects.
Genetics of obesity: The science is very clear now that there is a strong biological basis for obesity. This drug is yet another example of how finally the brain dictates how much you eat. I remember writing an article titled “Cause of obesity” 12 years back arguing for the powerful role of genetics in obesity. And as expected, it received a lot of push back then. Only around 1% of the obese take a weight loss pill. This is largely because of the prevailing ‘wisdom’ that obesity is a choice; a narrative that further drives the stigma that comes with obesity.
Conclusions
- The drug shows almost 15% weight loss - almost double the weight loss than any of the currently approved drugs.
- Side effects were mainly gastrointestinal, but long-term effects are unknown.
- $1250,00 for a month’s supply - an irresistible drug at an unaffordable price.
- Ending with a quote that sums up obesity succinctly, “Genes make the gun, while environment pulls the trigger.” Once-Weekly Semaglutide in Adults with Overweight or Obesity
- EPA: The omega 3 used only contained EPA and not the typical EPA + DHA combination that people often buy.
- Large dose: The dose used was 4 gms which is probably 5-6 times the dose of EPA found in typical store brand omega-3 supplements.
- As shown by these recent trials and meta-analysis, there is little benefit to the Omega-3 in people with heart disease and without. (for people with high triglycerides on statins, high-dose EPA could be beneficial)
- On the other hand, there is a very small increase in the risk of atrial fibrillation with omega-3 at higher doses.
- Looking at the benefits and risks, I personally wouldn’t take Omega-3 for heart health. Would you?
- Trials show fish oil to have modest benefits for folks with depression.
- However, in the general population or people without depression, no trials have studied if fish oils/ omega 3 can prevent depression or even improve mood.
- So the primary question was can fish oil supplementation (Omega-3) prevention depression or improve mood in people over the age of 50.
- Participants: Around 18.5K men and women (>50 yrs) with no symptoms of depression nor undergoing treatment for depression were randomized into 2 groups.
- Interventions: The intervention group took omega-3 supplements (1-g/d dosage of 465mg of EPA & 375mg of DHA) while the placebo group took a matching placebo for an avg. of 5.3 years
- Outcomes: The primary outcomes were risk of depression and mood changes based on questionnaires.
- Depression Increased: There were more depression events (651) in the fish oil groups (7.1%), while 583 (6.3%) events in the placebo group. Contrary to the study hypothesis, fish oils showed a statistically significant (p=0.03) 13% increase in depression!! (Hazard Ratio:1.13)
- Mood unchanged: The second primary outcome of a change in mood showed little difference between groups.
- Absolute risk: Although the researchers powered the study for a 15% “decrease” in depression and they saw a 13% increase, the absolute risk difference was only (7.1-6.3) 0.8%
- Natural frequency: A better way to express risk is through frequencies. So out of 100 people who took placebo, 6 will end the depression. And if 100 people take fish oils, 7 will end up with depression. So that means, one person more will get depression in 5 years!
- Numbers needed to treat: Or 125 folks will have to take fish oils for 5 years for one person to report depression.
- Strengths: Let’s start with strengths - huge sample size, long duration (5.3 yrs) and high supplement adherence (90%), 55% increase in Omega-3 in blood, pre-registered, double-blinded, and intention to treat analysis.
- Limitation: The major limitation is this was not the parent trial and hence all the participants (only 18.5K out of 26K) were not included. Although baseline measures appeared similar, unmeasured confounders could be a problem. So the certainty is low to moderate.
- American Heart Association (AHA) DO NOT recommend fish oils for people not at high risk of heart disease
- For people with existing heart disease, such as a recent heart attack, the AHA recommends approximately 1 g/day EPA plus DHA, preferably from oily fish
- AHA recommends one to two servings of seafood/ week for reduction of CV outcomes
- Clearly, the study does not support the use of fish oil / omega-3 supplements in adults to prevent depression or to have positive mood. So forget prevention!
- More importantly, fish oils showed an increase in depression, although the individual risk is small and of low to moderate certainty. (And a gentle reminder even supplements need to be rigorously tested in long-term trials)
- As always, the decision to take fish oil supplements for other benefits is an individual choice based on the risk, benefits, and your values.
- Pre-register: This means writing the outcomes/tests and statistical analysis plan, date stamping, and uploading to a public repository well before the data analysis. Pre-specifying your plan or registering helps prevent p-hacking: It refers to selecting outcomes or analysis that gives you statistically significant results (P value < 0.05). Or cherry picking favorable results!A simple example to illustrate the play of chance: Two archers: Archer A & B hits the bull’s eye! Who is the accurate archer? Of course, both of them.
- Example: Now what if I tell you that Archer B only got 3 attempts, while Archer B gets 20 or maybe 50 more attempts. Now you clearly know who is accurate. And this is exactly why you should pre-register our outcomes & analysis plan. The more outcomes and analysis, the more likely to get a significant p-value simply by chance.
- If you are doing a pilot or exploratory analysis, you do not have to pre-register. BUT results will be exploratory at best.
- In certain cases, if you report all the outcomes and perform a standard analysis, it should be fine. For example, if you investigate body composition changes and if you report muscle mass/fat free and body fat, you have reported all the standard outcomes there is to report!
- Get a statistician: Great studies will collaborate/consult with experts in their areas, hence the reason they end up great! For example, a study involving weight loss will include dietician or a nutritionist, and of course a few researchers who specialize in weight-loss interventions.
- A statistician, however, is required for every study. Every study involves sample size calculation and statistical analysis. Statistics are complex. The more I learn about stats, the less confident I am doing them on my own. And yes sir, this step should come prior to registering your analysis.
- Randomization & concealed allocation: You have to randomize participants into groups. Also, conceal it well so that neither you or the participant can predict and alter the sequence. For example, imagine I am investigating a new drug for COVID and a sickly person gets randomized to the drug group. I might be very tempted to move him to the placebo group because I don’t want him dying in the drug group and make my lucrative drug look bad! And if I did that, I break the randomization. In my personal experience, I never felt tempted to move participants nor participants ever requested to be put in a certain group. It is probably because none of my studies had a control group or/and exercise studies have little at stake. But this could change if I had a pet hypothesis or financial gains at stake.
- Intention to treat analysis (ITT): You have to analyze all the participants in the study. For example, if you exclude participants from the analysis for adherence, it is not intention-to-treat analysis anymore. If you exclude participants for lack of adherence, often seen in exercise & nutrition studies, the study is not ITT anymore and high risk of bias.
- Blinded outcome assessors: You have to make sure that people who test participants at the end of the study are not aware of which group the participant belongs to. This becomes even more important if the test is subjective. For ex, test of physical function in older adults are assessed using a stopwatch and can be easily influenced. I can easily encourage them or stop the time slightly ‘quicker’ in the groups that I want to improve! But objective measures like DEXA or death testers cannot influence the outcome. (All my RCT’s used blinded assessors)
- Use reporting gudelines:There are several studies that actually did everything right, but didn’t bother reporting in the paper. Consequently, they all end up as “some concerns” or “high risk of bias”.
- Reporting guideline have been developed for each study design to guide you on what to include in your paper. In my experience, reporting is probably the least work compared to all other aspects of a research study. So you have no excuse whatsoever not to report well.
- Share data: Upload your data once you publish the results. Or at least have it available upon request. This will enable reviewers (or the public) to check the veracity of your findings. For example, the recent retractions in NEJM & Lancet were possible because the reviewers requested the data, but the author declined, leading to further questions. Mind you, fraud is very rare in research, and most errors are honest mistakes.
- If you are a Ph.D student (or a researcher), are you sticking to these? If not, please start.
- If you read research to make important health/performance decisions, look for these simple rules to identify trustworthy research.
- Population: 151 individuals between 21 to 70 years with back pain for at least half the days of the last 6 months and with an pain intensity score of 4 of 10. And they had the pain for a mean duration of 10 years. So I would say people with moderate chronic pain.
- Intervention group: They were randomized to an intervention that involved treating chronic pain as a "brain-generated false alarm". The intervention shares some concepts used in modern pain science & cognitive behavioral therapy. The therapy involved 8 1-hour sessions twice weekly for 4 weeks. The treatment is about changing patients’ beliefs about the causes and threat value of pain.
- Comparison groups: The 2 groups were standard care (no treatment), and a placebo group which got a saline injection.
- Primary outcome: The primary outcome used a pain scale rating from 0 -10 measured after 1 month, and followed for a year.
- Pain reduction: The pain showed a large reduction in the treatment group compared to the placebo and usual care as shown in the graph here. Also these differences were maintained even after 1 year.
- Pain-free: 33 of 50 participants (or 66%) in the treatment group were pain-free or nearly pain-free (reporting a pain score of 0 or 1 of 10), compared with 10 of 51 participants (20%) randomized to placebo, and 5 of 50 participants (10%) randomized to usual care.
- Also, as expected, the reduction in pain was caused by changes in fearful pain beliefs/pain avoidance. Those with the largest reductions in beliefs that pain is equal to injury and those who started using the feared movements showed the most improvement. In short, these people turned down the threat or lowered their sensitivity.
- Single-center: The study was done at a single center by experts trained in these very specific techniques. I am not implying anything, but a number of authors had disclosed financial COI's. I would like to see this replicated a larger sample size, multi-center study by other groups.
- Placebo group: The placebo group used injection. Would the results have been the same if the placebo got 6-8 hrs of attention from the pain therapist like in the intervention??
- Control group: were asked to follow the Norwegian physical activity guidelines, which is apparently 30 min of moderate level physical activity 7 days/week. The activities included either walking/running, skiing and aerobics.
- High-Intensity Interval Training (HIIT): Exchanged two of the five 30-minute moderate intensity physical activity sessions each week with two HIIT sessions. 40 minute sessions, 10 minute warm-up followed by 4×4 minute intervals (3 min active rest) at about 90% of peak heart rate (RPE: 16 on the Borg scale).
- Moderate Intensity Training (MIT): Exchanged 2 of the five 30 min sessions with 2 MIT sessions: 50 minutes of continuous work, 70% of peak heart rate corresponding to an (RPE:13)
- No Difference: Unfortunately, the study failed to show a difference between the control group and combined (MIT +HIIT) group as hypothesized. Or showed a miniscule 0.2% difference in deaths.
- HIIT better: Interestingly, from the abstract, the authors states “a lower mortality ‘trend’ after HIIT compared with controls and MIT”
- Healthy participant bias: So the big question is why did the study fail to show a difference? According to the authors under “Limitations”, this was largely because the majority of the participants were healthy and active. For instance, 80% of the participants had a high level of physical activity before joining the study. And this meant there were way low number of deaths than the authors had expected. They estimated around 10% deaths (2%/year) in the control group, but ended up with 4.7%. They also expected a 10% reduction in deaths, but ended up with 0.2%!!
- I partially agree with the authors, but it just kills me to know that they didn’t think about it prior to planning the study. 90% of the elderly who show up for an exercise study are healthier and highly active than the general population. In fact, The LIFE study, a similar study, which looked at an exercie program in elderly for 3 years excluded high functioning folks to avoid this exact problem. To put it bluntly, even before they recruited the first participant, the study was destined to fail.
- Low adherence: Another limitation according to the authors was that only 50% of the participants were able to follow the HIIT protocol (same for MIT too). But in my opinion, the low adherence to HIIT is just a reflection of how hard it is for people to exercise at higher intensities. Also, the researchers say that the control group exercised at an intensity between HIT and MIIT. If indeed they expected a higher adherence/no cross-contamination, that just means the study failed to meet their intervention targets, which questions the implementation or the intervention fidelity.
- The missing pilot study: Could have they have done anything different? Yes. IMO, these are some of the very reasons why a pilot study is so crucial before carrying out large study. A major reason for the success of the LIFE study is that they conducted a 1-year pilot study with around 400 people that showed informed how many will get disabled, the adherence, side effects, and so forth.
- 49% reduction in mortality??: A 49% reduction in deaths in HIT compared to MIT sounds huge, but is it really? A better way to understand risk is using natural frequencies. So, out of 100 people who did MIIT, 6 died, while those doing HIT, 3 died; means there will be just 3 fewer deaths if people did HIT compared to MIT in 5 years. So just a very small/trivial reduction that many won’t bother worrying about!
- Large uncertainty: If you look at the confidence interval, this decrease in deaths could be as low as 1 death in 100, no difference, or it could be even an increase in deaths (7/100)!! This lack of precision or large uncertainty is concerning. So a small/trivial effect and that too very uncertain (or non-significant).
Exploratory analysis: HIIT compared to MIIT and control group are just exploratory analysis. In other words, these weren’t pre-specified in the protocol plan, not even as a secondary analysis. Considering the 3 groups and over 20 secondary outcomes, the statistical comparisons could be easily over 100! So these results could be erroneous and simply due to chance.
The fact that MIT showed a 26% increase in deaths (yes an increase) “trend” compared to control is ignored shows why this practice is called ‘cherry picking’ - selectively picking analysis that favors your conclusion, and is officially called a “spin”.- Drop-outs & side effects: Drops outs and side effects in exercise trials are important. Drop outs were 33% in the HIIT compared to 26% in the MIIT. This differential drop out (10% higher in HIIT) is concerning and could be due the higher-intensity, but no reasons were reported. Adverse or side effects are a major concern with higher-intensities in elderly and should have been a pre-registered, statistically analyzed outcome. But no major difference is seen in adverse events reported.
- Quality of life (QOL): QOL of life showed a trivial, yet significant improvement with HIT. Or not a big enough effect to really bother about.
- Based on the registered primary outcome, the study failed to show that intensity had any effect on mortality.
- What about HIIT? Contrary to the authors and popular media, based on the the exploratory nature of the analysis, the trivial/very small effect, and large uncertainty, we can only have a low or very low confidence in the results. You can save “10 minutes” of workout time, but you will have to endure the discomfort of higher intensity, and also risk a higher likelihood of dropping out.
- And all this means the decision to exercise at higher intensity to reduce mortality is more of a personal choice and cannot be offered as a general recommendation across the board. So pick the intensity you like please!
- Older people don’t care about muscle mass or strength, what they care about is can they carry out everyday activities, such going up the stairs, getting up from the toilet, and so forth
- An athlete don’t care about their 1RM or max strength or core strength or vo2 max or Lactate threshold; they care if they can perform in the field or improve their timed trial.
- People don’t care about fat or lipid oxidation, but actual fat loss.
- Cancer patients don’t care about tumor size or progression-free days; instead they care about survival or quality of life.
- Bodybuilders don’t care about EMG, protein synthesis or mTOR; they care about actual muscle size.
- RCT’s: As shown in the picture, randomized controlled trials are the most trustworthy. Why? The reason is that they are the only study design that can show cause and effect. Naturally, the study type, which can topple RCT’s is a collection of RCT’s called a meta-analysis. I hope now you understand why researchers are constantly calling for an RCT for drugs against coronavirus.
- Observational Studies: Observational studies are done for long term outcomes (death, cancer) and studying harms. But they can only show associations and not cause and effect, which is a long way to say, “we really don’t know if this is true, my friend, so be careful”.
- In-vitro /Laboratory/ animal studies: These are animal studies, studies looking at things in a test tube, physiological or mechanistic studies. Other terms for these are “basic science studies”, and as you guessed these are all surrogate outcomes. Most folks are thinking these type of laboratory studies when they think science/research.Apparently, a lot of what is taught in college/graduate/medical is at this ‘in vitro/physiological level’ without students really understanding/taught the inherent limitations. They believe that we have figured out all the mechanisms about “how things work” in the body. And most lay people are easily fascinated when they hear complex, mechanistic pathways and hard-to-spell names.
- Expert Opinion: The lowest is our beloved expert opinion. So just being a doctor or having a Ph.D may not mean much. And good doctors know this very well and will always talk about evidence or lack of evidence and will be very measured in their recommendations/talks.
- What type of study design is it? And where does it fall in the hierarchy?
- Did they use a surrogate outcome?
- Were the results clinically significant?
- Did they control for researcher biases? Good luck.
- High- Intensity Interval Training (HIIT): When the intensity is high (near maximal)
- Moderate Intensity: When the intensity is moderate.
- Sprint Interval training: Involves all out sprinting (maximal effort)
- Interval training and continuous training both reduce body fat percentage (%).
- Interval training provided 28.5% greater reductions in total absolute fat mass (kg) than continuous training.
- Have a base aerobic fitness before you jump on HIT. So continuous training for a few weeks before you start
- A 5 min warm up and few minutes of cool down
- Choose stationary cycle or elliptical. Avoid running on treadmills for safety
- Most studies had them perform 3 times/week
- Gradually progress out intensity
- Calorie restriction (or diet as they say)
- Physical activity or exercise (cardio & strength training)
- Behavioral approaches to improve adherence: Most people talk endlessly about the above two, and will completely miss the 3rd one. Unless you make behavioral changes to stick to your new dietary and activity patterns, you WILL gain most it back. Almost all weight loss recommendations include behavioral strategies. And almost everyone who has successfully kept weight off has knowingly or unknowingly made behavioral changes.
- Looking at the amount of fat loss, the study quality, time taken, and other above factors, I wouldn’t make any strong recommendation for either of the exercise modalities. Pick the one you enjoy the most and that you can continue for years.
- If fat loss (and keeping it off) is your goal, focus on calorie restriction & exercise and, more importantly, on behavioral stratergies so that you can stick with the above.
- If you are looking for a magic bullet for fat loss as the title claims, I have news for you: there isn’t one. 😊
- Relative Risk: Each additional half egg eaten per day (3-4 eggs/week) was associated with 6 percent higher risk of cardiovascular disease and 8 percent higher risk of any cause of death. That’s great, but what does 6 & 8 percent mean? Do 8 out of 100 people die or you are 8 % dead? A better way communicate risk to play people is through numbers need to harm or NNH.
- Numbers Needed to Harm (NNH): Using absolute risk, if 90 people have 3-4 eggs per week, one additional person will develop heart disease in 17 years (and his could be as high 312 people!upper limit of interval). For the outcome of mortality, this means 50 people have to eat egg to have one death in 17 years (and this could be as high as 90!). Now how does that sound? As you guessed it, the risk appears much less threatening. However, from a population perspective we are talking about thousands of people getting heart disease which is a serious public health concern. From what I have seen, none of the major articles have managed to communicated the risk properly. Understanding the risk well is is an important aspect of an evidence based approach.
- Any relation with Cholesterol: It should be noted that the study observed a similar increased risk with an increase in cholesterol intake. Apparently, the association between eggs and heart disease and mortality disappeared when they adjusted for cholesterol, showing that it could be the cholesterol in eggs that may be the problem.
- If you have a high cholesterol levels, it may help cutting back on egg yolks. However, if your cholesterol is low, eat them.
- If you are living in another country, like India or UK, do remember that the average cholesterol levels are much lower than in USA and these results may not apply.
- If you eat 2-3 eggs per day and a lot of meat, it may be better to cut back on eggs or maybe have egg whites instead.
- To date, there is little evidence to show that using a training mask improves endurance or strength training performance.
- Further, limited evidence show that the mask can negatively affect your acute weight training performance that may lower your gains in the long-term.
- If you want to improve performance by training your breathing muscles, respiratory muscle training is a far better option.
- Lack of studies: There is lack of studies looking at the effects of frequency on muscle growth and strength.
- Anecdotal Evidence: High-level weightlifters split their training volume into two training sessions in an effort to maintain the intensity.
- Untrained subjects: Most of the studies on frequency used untrained subjects.
- Population: Trained college-aged men (18-30 years) who were actively participating in resistance training for a minimum duration of 6 months (minimum of 3 days per week). That is, 1RM of 125% of their bodyweight, a bench press 1RM of 100% of their bodyweight, and a deadlift 1RM of 150%. So I would say intermediate lifters.
- Exercise Program: The exercise program is shown in table below. The volume was equated and 6/week sessions lasted an hour, while the 3/week sessions lasted approximately 2 hours. The training focused on the main lifts as shown in table, but the subjects also performed exercises for biceps, triceps, lats, shoulders and such.
- Outcomes: Strength using 1RM testing for the major lifts and body composition using an A-model ultrasound.
- Sample size: They randomized 43 men into two groups.
- Strength: There was no significant difference in strength between the groups for bench, deadlift and squats.
- Body composition: Fat-free mass and fat mass also showed no significant difference between the groups.
- First, you cannot prove the null hypothesis; you can only disprove it. I have seen this error in a number of studies during peer review. If you do want to show equivalence, you have to use a non-inferiority or equivalence study design.
- Second, a study is conducted when an intervention is hypothesized to be superior than the comparison group. Or the intervention is cheaper/practical/ less side effects compared to the comparator even though it may not be superior. Why conduct a study when you know the 6/wk takes more time and is more burdensome but still not better than a 3/wk frequency?
- Do drop outs matter? Imagine a weight loss supplement study that randomized 5 subjects to a control group and 5 into the diet pill group. At the end of 12 weeks, the diet pill group lost 5 lbs while the control group lost 2 lbs, and the difference was statistically significant. So the diet pill works! Now imagine, if I say 3 dropped from the weight loss drug group because they didn’t lose any weight. So if we had somehow tested them and included them in the analysis, the weight loss in the weight loss group would be 2-3 lbs and not 5lbs. That means, the weight loss drug is clearly not effective and is the truth! So drop-outs do matter a lot.
- Intention-to-Treat: The technical term for including all the participants in your analysis is called Intention-to-treat (ITT). If you only include the participants, for example, that showed up for at least 75% of the sessions or adhered to the exercise protocol, then the analysis is called ‘per protocol analysis’. ITT is the preferred analysis for all the leading medical journals. I would say 98% of exercise studies ignore the ITT principle. In my previous study, I report my results both in ITT and per protocol formats.
- Anecdotal evidence: In fact, one large reason why we cannot trust anecdotal evidence is because they don’t count the negative hits. All the glowing testimonials are only coming from people who are alive and doing well. But the people who are dead or struggling in bed do not come back to say ‘thank you’ and hence forgotten. A scientific study, on the other hand, takes into (or should take into) account both positive and negative results.
- Pick one body part or a lift and try it;not every lift or muscle group as in this study.
- Or have medium effort or light effort days like many programs than going at 100% intensity every day.
- Do not go to failure on high frequency programs. Did they do in this study? I have no idea since they did not report it.
- You can use high frequency to either spread your weekly volume or get more volume depending on your current program.
- Just so you know, most of the gains made during a high frequency cycle may not stick when you climb down to a regular routine.
- The study showed that a 6 days/wk program is NOT better than 3 days/wk program to increase muscle mass and strength in intermediate lifters in 6 weeks. And considering the large drop-outs in the high frequency group, it is highly likely that high frequency could be worse.
- Learning Tip: Next time when you read a study, check how many dropped out from each group and how it could have affected the results. Also, next time you hear a glowing positive review of a program or diet, think about how many negative reviews that were missed.
- On average, 40% of people will be diagnosed with cancer in their lifetime
- Although several cancers are genetical, most of them are due to environment and lifestyle
- The committee reviewed almost 45 reviews, meta-analysis and pooled studies
- Strongest evidence linked highest versus lowest exercise levels to reduced risks of bladder, breast, colon, and other common cancers (by 10-20 percent)
- Limited or moderate evidence exist for other cancers
- Not clear about brain cancer
- Some evidence for sedentary time (or sitting time) associated with cancers risk
- Limited evidence to show exercise reduces mortality in cancer survivors (people who had cancer and survived)
- Currently, large studies going on to see if exercise has an effect in cancer survivor’s (ex., CHALLENGE trial)
- There is a dose response relation, but exact dose of exercise not clear, varying age groups, and so forth?
- All these results from observational trials. So we need some large RCT’s
- We need to know more about the dose response or whether moderate intensity activities such as walking are sufficient and whether resistance training has a role too.
- almost 10% of the population in the US have diabetes; almost 34% are pre-diabetic (1 in 3 people)
- 90-95% of the cases are Type 2 diabetes
- 2-4 times likely to have a stroke or heart disease
- number one cause of blindness, amputations, and kidney disease
- seventh leading cause of death.
- Previous Studies: Previously studies have shown lifestyle interventions (weight loss, physical activity, and healthy dietary choices) can prevent or postpone type 2 diabetes in people who are pre-diabetic (high blood sugar but not diabetic yet).
- Current Study: In this study, they wanted to see if weight loss could reverse diabetes in folks who are diabetic and taking diabetic medication. Is it too late for them?
- 298 patients (aged 20–65 years) diagnosed with Type 2 diabetes (within the past 6 years) and taking medications were allocated to a weight management program (n=149) or a control group (n=149)
- The intervention group had a very-low-calorie weight loss diet 825–853 kcal/day diet for 3–5 months, followed by structured food reintroduction and weight loss maintenance phase.
- This was a pragmatic trial meaning the intervention was offered by primary care doctors and not at specialized research centers as is often seen in big studies.
- Weight Loss:As shown in the graph, Diabetes reversal was strongly associated with body weight or body fat lost. So weight loss should be the primary goal of treating diabetes.
- Weight Maintenance: That being said, almost all weight loss studies have struggled when it comes to the weight maintenance aspect. So the real test is if they can keep the weight off and thus diabetes after 3-4 years.
- At least based on this study, Type 2 Diabetes is not a permanent, lifelong condition.
- If you are pre-diabetic or diabetic and don’t want to take drugs, weight loss might be your best option.
- Of course, consult with your doctor if you are planning to lose weight.
- You slowly lose the ability to move and function, leading to physical disability
- You have a higher risk for falls. Falls in older adults can be very debilitating, especially if the falls results in a hip fracture
- Low muscle mass may also lead to institutionalization, hospitalization, and mortality
- Lack of physical activity
- Decrease in anabolic hormones, like testosterone, GH
- Increase in age-related inflammation
- Decrease in food intake and protein intake
- Original Definition: The first definition defined sarcopenia as muscle mass that is two standard deviation below the muscle mass of healthy young adults. Although this was fine for scientific purposes, for clinicians this wasn’t good at all. FDA and regulatory agencies don’t care about changes in muscle mass; they want to see changes in meaningful endpoints such as physical function or falls. For example, the FDA only approved bone density drugs when it showed it could decrease fractures from falls and not just an increase in bone density.
- Second Definition: The second definition was a major departure from the first definition; the new definition included loss of strength or performance in addition to the already included low muscle mass. This came through from a major realization that muscle mass is only weakly related to physical function in older adults compared to muscle strength. In fact, I am proud to say that my current mentor (Dr. Todd Manini) is largely responsible for showing this disconnect between strength and muscle mass in older adults. His papers introduced the term Dynapenia (loss of strength) and stressed the point that loss of strength should be the focus than the loss of muscle. As a result of his work and many others, the definition of sarcopenia now includes low grip strength and/or walk speed, in addition to low muscle mass.
- Latest Definition: Although the definition certainly improved, there was one major problem: The previous criteria or cut-offs for grip strength or muscle mass was based on single studies, which is not data driven or evidence-based. This prompted the NIH ( National Institute of Health) to create the sarcopenia project in 2010. The sarcopenia project combined 9 large, diverse studies (almost 25,0000 participants) to come up with cut-offs for grip strength and muscle mass to identify sarcopenia.
- ICD Code: Recently, after much campaigning, CDC has finally established an ICD (International Classification of Diseases) code for Sarcopenia. ICD code is used extensively to classify diseases, and other health problems Establishing an ICD code means that clinicians, policy makers, researchers can now treat sarcopenia as an actual disease/condition than some vague condition that is talked about
- Grip strength is measured using the Jammar dynamometer (<16 kg for Women and < 26 kg for Men).
- Muscle mass is measured using DEXA
- Drugs: Currently there are no drugs approved to prevent muscle mass loss. Testosterone administration has shown to increase muscle in older adults, but the improvement in strength or physical function is inconsistent. .Also, there are some cardiovascular and prostate cancer risks associated with testosterone supplementation .
- Exercise: Exercise has shown to delay or prevent the loss of physical function. Currently, strength training is the only effective strategy to increase or preserve muscle mass.
- My personal opinion is that just like you don’t wait to see if you have a higher risk of getting lung cancer if you smoke, you shouldn’t wait till you have been diagnosed as sarcopenic to start exercising. There are so many benefits to exercise and increase in muscle mass just happens to be one major benefit.
- Bone density drugs are usually prescribed to prevent fractures. But what many people are not aware is that the majority of fractures are due to falls. And low muscle strength is a major risk factor for injurious falls. So if your bone density is low and you are worried about fractures (and you should be), preventing falls makes more sense to me than just increasing bone density. Most people talk about strength training as a way to increase bone density to prevent fractures, but the increase in muscle strength may be more important when it comes to preventing fractures. ·
- Grip strength is obviously cheaper than getting a DEXA., which could cost a couple of hundred dollars. However, if you try your grip strength (and most gyms have a grip strength tool)you have to make sure you are using the Jammar dynamometer. They are the gold standard.
- Remember as you go past 40, you will start to lose muscle mass
- This loss of muscle may lead to some dire consequences, such as loss of physical function, hospitalization, and falls
- Like it or not, the only effective way to minimize muscle loss is through exercise, especially strength training.
- Mortality: Low levels of cardiovascular fitness is associated with greater mortality and heart disease. In short, if you can improve you CRF you will live longer. The graph here shows death rate decreasing stepwise with increasing CRF
- Risk factor: It is potentially a stronger risk factor to predict mortality than established risk factors such as smoking, hypertension, high cholesterol and type 2 diabetes. In short, even if you are obese and have other risk factors, if your CRF is high you may mitigate some of the problems of obesity and smoking.
- Chronic diseases: High CRF is associated with low levels of cardiovascular diseases as well as reduced risk of Dementia, Alzheimer’s, Diabetes, other diseases. Also, associated with lower risk of developing certain cancers, including lung, breast cancer and gastrointestinal cancers
- Cardio: Cardio here includes both heart and blood vessels. Just like you can make your muscles stronger by weight lifting, your heart muscles can also get stronger too. Further, your blood vessels become more elastic and less clogged with exercise.
- Respiratory:Means lungs and breathing muscles. A higher CRF means your breathing muscles are stronger, and you have more capillaries for better O2 and Co2 exchange.
- Muscles: Muscles in your body are also involved in CRF too. Higher CRF comes with more number of capillaries in the muscles (means more blood supply and better waste removal and nutrient transport) and more mitochondria (better oxygen extraction) in the muscles.
- Endurance exercise: Anything that can increase your heart rate will increase your CRF. So exercises could be in the form of walking, brisk walking, jogging, playing sports, swimming, climbing stairs and such. All you need is a pair of legs!
- Low Fitness: If you think you get easily tired and may not do good, then you are in luck: The greatest benefit of CRF is seen among people who have a low level of CRF! So even 10 min/day of walking can increase CRF.
- Intensity: The greater the fitness level, harder the CF improvements and higher the intensity required. CRF is more responsive to intensity than frequency or duration. In short, if you have always been exercising, focus on walking faster or increasing your intensity of exercise.
- Strength training: Strength training, as we know, do not increase your heart rate enough to make a significant improvement in CRF.
- Diet: All the apples, organic foods and a healthy diet will not increase your CRF.
- Measurement: In this test known as Vo2 max/peak test, you will have to wear a mask and walk/run on a treadmill until you are basically pooped. This is the gold standard test and directly measures how much oxygen you are using. The vo2 max/peak number could range from 10 to 80 ml.o2/kg/min. Exercise science departments in most universities do provide this service for a fee
- Estimation: You can estimate your max/peak vo2 but they often comes with errors (10-15%). You can exercise at a submaximal intensity and then estimate your peak max vo2 using the heart rate obtained. For example, cycle ergometer, 1-Mile walk test, or 6 min walk test. Most fitness centers include this in their fitness assessment.
- Equation: You can also predict it solely using equations without any exercise using BMI, heart rate and so forth. Here is one: https://www.worldfitnesslevel.org/#/
- 1. in short, If you are overweight, even if you are not losing weight/fat, be aware that exercise may attenuate some of the risks of obesity via the improvement in your CRF.
- 2. If you are a trainer, please routinely measure your client’s CRF and focus on improving it than just strength and muscle/fat.
- 3. If you ever wanted to live longer, improving your cardiorespiratory fitness by exercise maybe the single most important thing you can do.
- 4. Finally, please share this with your friends and family .
- Multicenter study involving 49 countries and nearly 27,000 subjects followed for 2 years. How is that for sample size?
- The drug ‘Repatha , already approved by FDA, is injected twice a week. How much does it cost? Around 15K per year!
- The outcome was a composite score of occurrence of heart disease, stroke and such.
- What was the result? The drug lowered cholesterol by nearly 60% which is almost unheard of. And we are talking about people who are already on statins. But the outcome showed only a 1.5 % difference between the drug group and control group. Although, 1.5% appears very low, this could translate to benefits to millions of people. Interestingly, there was no change in mortality.
- There was no difference in adverse effects. But studies looking at cognitive function and cataract are still ongoing.
- US National exercise recommendations/guidelines recommends BOTH endurance activity and strength training. And this is true even for global exercise guidelines by the World Health Organization (WHO).
- Why cardiovascular activity is considered more beneficial than strength training for improving mortality and preventing chronic diseases ? It is simply because not ten’s, not 100’s, but thousands of studies, which have shown improvements in mortality and diseases like cancer, cardiovascular disease, diabetes, cognition and health are largely from endurance type of activities like walking, cycling, jogging, running and such tasks.
- Joint pain and injuries by weight training 6 days per week or for 3 hours a day by a few bodybuilders/competitive lifters is NOT a compelling argument against 2-3 days per week for 30-60 min of strength training, right? So using examples of cyclists and marathon runners who perform hours and hours of high-volume endurance exercise and comparing to 150 min moderate intensity/75 min of vigorous activity per week is just missing the boat.
- A small number of studies in untrained do show circuit training (type of strength training) to improve cardiorespiratory fitness. But these always include very short rest times 0-30 sec and higher repetitions. Long-term improvements are questionable and practical/safety issues become very real when using free weights with shorter rest time. A strength program recommended by the author with 5 sets of 5 reps and 3-5 min rest times is certainly not going to help your cardiovascular fitness. Guaranteed.
- Very recently, the American Heart Association (AHA) released a scientific statement.(keep in mind that these statements are only and only released when the body of evidence is large, high-quality, compelling, and have significant public health impact) It says cardiorespiratory fitness is a potentially stronger predictor of mortality than established risk factors such as smoking, hypertension, high cholesterol, and type 2 diabetes mellitus and it should be routinely assessed. This is huge if you are someone who happens to like staying healthy and living longer. And guess what’s the best way known to mankind to improve cardiorespiratory fitness? By cardiovascular or endurance exercise.
- Finally, what many people, including the author, fail to understand is that a moderate intensity activity could be just brisk walking and vigorous intensity could be as simple as race walking/jogging/cycling/playing sports. So no guideline is ever asking you to run a marathon or on a treadmill forever as you often see folks do in the gym. Will CV exercise hinder strength gains? It may depending on a lot of other factors (frequency, type, intensity, duration), but you have to remember that these guidelines are meant for overall health and well-being and not for people who are paranoid about their 1RM squat numbers or losing muscle. If you belong to the latter, it would be easier (and wiser) to either accept the trade-offs or change your priorities rather than trying to change THE national guideline.
- diagnose the problem (for example, why can’t this person squat deep, how to correct exercise technique, why he/she is not gaining strength or losing weight.),
- search for the relevant research evidence (how many sets to gain muscle for an advanced trainee, or which exercise targets specific muscles) and critically analyze the research evidence for methodological issues (was the study in beginners, was the outcome measured relevant)
- understand both the benefits, the risks involved, and other alternative approaches to the goal (a Crossfit type workout might be motivating and improve general cardiovascular endurance, but has a high risk of injuries)
- alter the program based on the client feedback and results (reducing the number of sets or modifying the exercise (angles, ROM and do forth) for an older person or someone with pre-existing shoulder injuries• .)
- Listen and understand clients value and preferences, clearly communicate the risk, cost, benefits in a simple manner, and use a shared decision approach to come to a decision
- First, as shown, the different types of evidence are arranged in an orderly fashion. As we go up the hierarchy, the trust or the confidence we place in the study results go up too. RCT’s are the most valid research design, as they allow the ability to infer causality. And expert evidence is the least trustworthy and occupies the bottom position. Meta-analyses- a collection or a group of RCT’s-are generally considered the highest form of evidence, as they synthesize the entire body of literature on a given topic and quantify the results based on a statistical measure of practical meaningfulness. Meta-analyses can be particularly important in exercise- and nutrition-related topics, as the sample sizes are often small and thus pooling the data across studies provides greater statistical power for inference.
- Second, it is important to note that depending on the quality of the study, an RCT can be downgraded, too. A poorly designed study will never provide a high level of evidence, and in fact can impair the ability to draw proper evidence-based conclusions. The hierarchy therefore is not set in stone.
- Third, there is always evidence. So the best available evidence is what is available and need not come from an RCT (Randomized Controlled Trial). But based on the type of evidence, our confidence in the results and our recommendations will differ accordingly.
- Example 1: If a client comes with a new program that uses 5 lb weights to increase strength, we know from basic science that without load progression, muscle and strength gains will be nil. Such a program would go against the most fundamental theory of muscle growth. So you can make a strong recommendation against the program, even without an RCT.
- Example 2: Recently, the Ebola virus vaccine was used before conducting an RCT. How is that possible? Here is a classic example of weighing the benefits, risks, alternative approaches, and making a strong recommendation with weak evidence. In this case the risk is death, the benefit is obvious, and there are no alternative approaches. Thus, the risk/reward strongly favored giving the vaccine. And 99% of the informed patients would agree with the recommendation.
- Example 4: An observational study shows that eating meat raises cancer. Considering observational studies are lower in the hierarchy no matter how well the study is conducted, recommendations cannot be more than just suggestions.
- First, even if you gain benefits with a certain program, in many cases, it is extremely hard to figure out what was the variable that made the difference. Was it the specific exercise, the change in diet, the placebo effects, genetics, or some unknown variable?
- Second, it may not be clear if you are indeed making an improvement depending on the outcome. For example, gains in muscle come very slowly for trained individuals (like years for a several pounds). Hence, you will have to run a program for a few years to see if it works or not. However, controlled research often uses measures that are highly sensitive to subtle changes in muscle mass, and thus can detect improvements in a matter of weeks.
- Not dieting: This graph based on your body weight measurements when you are NOT on a diet or when you are NOT trying to change your weight. Hence this your typical or default changes in weight. These weight changes could be due to skipping meal, on a trip/vacation and having too much food, water weight changes, measurement error, being sick, working too hard, and so forth.
- High Probability area: The high probability area in green color represents of the middle of the curve. As you can see majority of the time in your life your weight loss is around +3 to -3lbs. That means, there is a very high probability that majority of the times your weight loss/gain in the +3 to -3 lbs. The weight fluctuations in this area could be just water weight or measurement errors or missing a meal or so forth.
- Low Probability area: The low probability area in red color represents the tail end of the curve. As you can see, only a few times in your life your weight loss/gain as high as 5 lbs. That means, there is a very low probability that your weight loss/gain is 5 lbs or more. Those were the times when you were sick and lost weight or went on a vacation and gained a lot of weight or due to dome other unknown reasons.
- Truth: A scientific study is conducted to find the truth. Although we will never know for sure if we have found the truth, we know that the better the study methods, the closer we are to the truth.
Bias: In scientific terminology, any deviation or distortion from this underlying truth is called bias. When you have a high risk of bias or deviation, we can never be confident or certain of the results.
- Randomized Controlled Trial: The very reason why RCT’s or randomized controlled trials are considered to be the gold standard is because of the low risk of bias inherent to these types of designs. Rightly so, only RCT’s can show cause and effect - or if X causes Y.
- Randomization: Randomization simply means that every participant had an equal chance to fall in either of the two groups. Randomization ensures both groups are balanced before the start of the study. This is the most critical aspect of an RCT. If they did not specify this in the study, you can safely ignore the study.
- Concealed Allocation: If a randomization sequence is generated, the next question is how were the subjects allocated according to the sequence. The allocation should be performed such a way that the study personnel have no clue who goes into which group or the forthcoming assignment.
- Blinding: In double blind, the participants are not aware if they are taking the drug or the placebo. Also, the testers are not aware which group the participant belongs to. Hence the name double-blind. In exercise study, participants obviously cannot be blinded, but testers can and should be blinded (called single-blinded).
- RCT’s: During my Ph.D, I did 3 RCT’s. Except for my first study which had no concealed allocation, all of them were blinded, randomized, and maintained concealed allocation. In fact, I explicitly stated the lack of concealment in my first study. My last one had ITT too. Being a student, it is hard to dictate the study conduct, but I am proud that I managed to do them. What I have come to realize is that unless you run a study or two of your own, you will never know the importance of these quality controls in research.
- Example: Let’s take the example of blinding: Unless your outcomes measure is death or something very objective, almost all measures are subject to bias. For example, one of the popular tests to measure physical function is Get up and Go test. For this test, they have to get up from a chair and walk around a cone a few meters away and sit back as fast as they can. They get two trials usually. I can easily make them beat the their first trial by simply saying ” now try to beat the time for the first trial”. If It didn’t say, they generally don’t. Or when I measure strength, I can easily give the group which I want to improve 2 more attempts to increase their 1RM. Some of the other measures I could have done to reduce bias: trial pre-registration, and blinding of the data analysis. Compared to other trials, trials involving exercise are extremely hard since you are supposed to train subjects 3-4 days per week for 16-20 weeks. So I admit that the logistics of ensuring blinded trainers and testers are easier said than done. But that’s no excuse.
- Replication: A scientific study is conducted based on the inherent assumption that the results will be the same if we repeat the exact study. What is the point of doing a study if we cannot repeat the results, right? Guess what, we are realizing that we just cannot replicate majority of our studies. Some popular examples:
- In 2012, 270 scientists tried to replicate 100 of the psychology studies published in the top 3 journals (Open Science Collaboration). And how many could they replicate? 39 out of 100. Now imagine replicating the studies in the bottom-tier journals?
- What about medical science? Amgen cancer research tried to replicate 53 ‘landmark studies’ in cancer biology. They replicated 3. Bayer tried the same and could not replicate 65% of them.
Lack of Quality: Why this crisis? There are number of reasons raised: small sample size studies, problems in duplicating the methods of the original study, conflict of interest, looking at multiple outcomes and reporting the significant ones, suppressing negative results and so forth. As many have said before, a large reason why there is a crisis is simply due to the lack of emphasis on the methodological quality of the studies. Unfortunately, the emphasis is purely on statistical significance or lack of it. In fact, 96% of the articles indexed in Medline from 1981 show a statistical significant result. That means, out of 1000 hypothesis scientists got almost 960 of them right!
Incentive for Science: In my opinion, the root cause for the lack of quality goes back to how science is rewarded.
- Journals get more citations and readership with ‘significant’ findings.
- Researchers’ chances of getting grants improve with significant findings. Mind you, for some professors and researches in big universities, salary and staying in job is dependent on if they can bring in grants.How about that for pressure?
- Graduate students are praised for their productivity. I have been called productive a number of times (a term which I dislike). I have never met anyone who spoke a good word about the quality of my studies and reporting nor emphaise the importance of quality. The more studies, the better your CV looks. So the last thing a student is worried is about is his/her study quality.
- Rankings/Impact factor are based around citations which goes back to ‘significant’ findings
- No reward for replications. No journal cares about publishing replications. It is not hot news.
Unless we change how science is rewarded, we may not change anything I am afraid. A good study can take time ( maybe years), but is well worth the time. Thank you for all the likes when I post my studies on Facebook, but I am sorry to say that any study can be published these days. There are 100’s of journals in each field.
- Reviews: Reviews of scientific research perform a very important job. A review should serve as the Robin Hood for readers/practitioners in that field by rigorously analyzing and exposing the flaws that the peer review overlooked. Critical analysis is THE most crucial aspect of an evidence-based approach. And it’s especially important in a new field like exercise science, where journals hardly care about quality. I have done it too, but just explaining the study and reporting nice-looking graphs is not a review - it is just a study ‘summary’.
- Researchers should focus on improving the quality of study conduct and reporting.
- Graduate students should be educated on the importance of study quality and not on ‘productivity’.
- Ranking and reward structures should be built around study quality rather than ‘significance’.
- Readers should look for these quality criteria first, and then look at results.
- One study can never be definite, no matter who did it or where it got published.
- Remember, all this above talk about replication, quality, randomization, methodology… is all about finding that elusive truth. And the best method known to man to find the truth is SCIENCE. So none of what I wrote undermines science or scientists; it is just my honest appraisal of where and how we can improve science.
- Decline in Power: In older adults, power declines at 2-3 times faster rate than strength.
- Functional Correlation: A number of studies have shown power to explain more of the variance in physical function compared to strength. In fact, 12 out of 16 studies showed muscle power to be slightly more correlated with physical function compared to muscle strength.
- Velocity Specificity: As dictated by the specificity principle, if you want to improve your squats, do squats. Likewise, if you want to move fast, you have to train fast.
- Power: Majority of studies have shown an increase in power using power training compared to traditional resistance training. For example, the study in our lab showed a 41% increase in lower body power in the power group, while the hypertrophy group showed a 17% improvement in aging adults. Great, but what about things that really matter like physical function?
- Functional Performance: Systematic reviews and met-analysis (or collection of studies) have shown power training to be more beneficial (small to moderate effect) than regular strength training in improving physical function.
- The majority of studies used power training with pneumatic machines. Pneumatic machines use air pressure instead of plates and are specifically designed to perform high-velocity training smoothly and safely. The funny part is that these machines are only accessible to researchers and high-end athletic facilities. Check the picture (A cylinder with compressed air instaed of weight plates)
- Of late, power training studies have been performed using standard plate-loaded machines that are often seen in gyms. And no major adverse or serious events have been reported.
- My latest study (in review) compared pneumatics and plate-loaded machines and showed that both to be effective and safe.
- I think this is an important aspect of research that is unfortunately overlooked by many articles and discussions.
- As is typical of exercise studies, most of the studies were of low to moderate quality. Hence the conclusions from these studies should be interpreted accordingly.
- Power training is one of those very few training programs that have a lot of theoretical and empirical evidence, yet still unknown to the majority of the personal trainers and older folks
- Since all you have to do is simply lift the weight faster, you can easily integrate power training into your current routine.
- As they rightly say, “wanna move fast, better train fast”
- If you know of any older person who lifts weights or exercise, share this article please.
- Exercise group: The exercise group of 818 subjects performed walking, strength training, balance, and flexibility training for 2.6 years. No special equipment’s were used for training.
- Control group: The control group of 817 subjects attended health education workshops .
- If you are past 50, there is steady decline in muscle mass and strength that has a detrimental influence to your physical function and independence, and thus quality of life.
- The only effective strategy to delay or minimize this decline in physical function is just regular exercise.
- To put it simply, if you are over 50 please start exercising. And if you know anyone who is over 50, please send this article to them.
- Start the cycle with high reps and culminate with low reps such as Week 1: 10-12, Week 3-4: 8-10, Week 5-6: 6-8: Week 7-8: 1-3 reps
- Perform a strength program with low reps for the big lifts such as bench press, squats,deadlfitsand shoulder press. And then follow with high reps for assistance exercises like dumbell press, rows and so forth.
- Or just do a pyramid, starting with high reps such as, set 1: 10, Set 2: 8, Set 3: 6 Set 4: 4.
- From a purely muscle growth or academic standpoint, we might have to wait for a few more studies to definitely conclude that high reps are not superior to low reps or high reps and low reps are equivalent for muscle growth. As of the current study, the likelihood of high reps being superior to low reps is low.
- From a practical/safety/volume perspective, it is better to rely on high reps more often than low reps. You can also mix repetition ranges, if strength is a concern.
- Study 1: The participants in this the study were touched by a cold piece of metal (-20) to evoke a nociceptive response. They were also visually shown one of two colored lights, either red and blue. Before being touched, it was explained that the light was very related to the cold stimulus. Now what did they find? Although the stimulus was identical, 8 out of 10 subjects felt more pain when the red light was shown than blue light. If you think about it, we have learned that red always signals danger. Though there were individual variations, it was very clear that the color of the light changed pain, but not nociception. The nociceptve fibers evoked the same response (as seen by C & A delta fiber activity) under both conditions, but the pain dramatically differed 2 .
- Study 2: Here the subjects placed their head in a sham or fake stimulator and were told a current would run through their head. They were told that the pain will increase as the intensity of the stimulation goes up. As expected, the pain went up as the stimulation went up even though there was no stimulation to begin with. This is another fascinating example of pain without nociception. http://www.ncbi.nlm.nih.gov/pubmed/2038488
- Each horizontal line represents each study. The year the study conducted is shown on the left. The shorter the line, the greater our confidence in the results
- The vertical line is the line of ‘no difference’. It means if the horizontal line touches the vertical line, the result of the study is not statistically significant or there is no benefit of the treatment
- As you can see only 2 studies ( in green) are significant, whereas 5 studies ( in red) are not significant. In other words 2 studies shows there is a benefit while 5 studies shows there is no benefit. If you just go by that, the studies are indeed conflicting and corticosteroid treatment is clearly not effective!
- Studies that do appear similar, may be different in some fundamental aspects and shouldn’t be compared.
- Instead of cherry picking individual studies to fit your conclusion, look at the totality of the evidence.
- Studies that are indeed similar and conflicting should be grouped together using a systematic approach called meta-analysis or systematic reviews.
- Midlines stabilization and organization
- One-joint rule
- Laws of torque
- How to stand: Whether you are at work, chatting with a friend in the grocery store, or standing in attention, your basic set up is always the same : feet straight, back flat, belly tight, head neutral, and shoulders externally rotated in stable position. Don’t be that guy who stands with arms crossed, shoulders rolled forward, back slouched, feet angled out etc… The takeaway is that: standing is a technique in and of itself… you need to practice the bracing sequence and remain conscious of your position all times.
- How to Sit: For starters, learn how to sit. Sitting - like standing - is one of the most technically challenging things we do? Yet most of us are clueless when it comes to sitting well. ..Once seated you need to keep at least 20 percent tension in your abs to maintain a rigid spine. It’s almost impossible to remain in good position for anything longer than that. I know - this is a huge pain in the ass and not always possible. But if you want to heal your body and reach the performance goals, you have to do the work. You have to make sacrifices. So pony up!
- Few Questions: For the newcomers. Pain has very little do with your posture and how well you move. There are 1000’s of people who have bad posture and have no pain. There are 1000’s of athletes running around with bad movement and no pain. There are 1000’s of cerebral palsy and polio patients walking around with the worst movement and posture and no pain. Mike Boyle popularized the joint by joint approach concept developed by Gray cook: joints have specific tasks and if it is impaired, the joint next to it takes up the slack and then you get injury and pain. If that’s the case, I would love to see what the blade runner (the double amputee, or any other amputees playing sports) has to say about his career. He has 2 joints missing and he still runs faster than 99% of us and has no pain! The only pain he has is that his wife is dead, and many doubt even that pain. It has been clearly shown in research that people are full of dysfunctions; a lot of people have disc herniations, spinal stenosis, and arthritis and yet have no pain. And then there are people who get treated for their dysfunction and voila the pain goes away - and guess what -the dysfunction still remains. This was all based on the biomechanical model of pain which is now outdated, unscientific and incomplete. If these questions intrigues you even slightly, please read my article on pain.
- What is the harm? A good question is what is the harm? I wouldn’t be bothered much if this was like another training method to make you bigger, faster, or stronger. My stance has always been we don’t have much evidence for the best program and there is no harm in trying it out for a few weeks. But this is way different: The problem here is that these recommendations which are re-enforcing people’s belief that the pain comes from bad movement and posture are just exactly what modern pain science has shown to be the problem. The more you talk about biomechanics, joints and movements, the more you are raising the threat level in the brain and making the pain chronic. This is exact reason why current pain science involves educational sessions to change people’s belief about the role of their muscles and joint in pain. Just changing the beliefs about pain has been now shown to lower pain, disability score and improve ROM and movement (1). How cool is that?
- Movements: In movements, he shows how different weight training exercises are done and how to do it right based on the above 3 rules. If you are not doing it right, it is either your flexibility or motor control or both. The majority of the stuff is nothing new and most lifters know this. He just lays it out in an organized manner which I like. He brings in some finer points with which you will find a lot of disagreement among the experts. For example, Kelly says the feet should be neutral when you squat or whatever. If your feet is turned out, the arch collapses or the knees can buckle in and hence result in energy leaks. The majority of lifters turn the feet out when they squat. Gray cook thinks that when you do loaded squats, feet should be turned out and he is another movement expert. Mark Rippettoe -one of the popular lifting coaches- says you should keep your head down when you do squats. My point is not to show you should do it this way, but besides the theoretical biomechanical masturbation and the usual ‘I get results’ to ride along , there is no evidence for some of these finer recommendations.
- Systems: In systems, he shows a lot of mobility exercises and mainly a lot of foam rolling using lacrosse balls and such. And his shot of fame was primarily through these videos of mobility exercises with bands to improve ROM and pain. These joint mobilization/wrapping techniques have been used for years (mainly from Brian Mulligan). So the question is are these beneficial? It is reasonable to advise people to avoid overloading the end range of motion and to maintain a healthy joint range of motion. Outside of that, we don’t have any solid evidence to show that we can prevent or predict injuries. If you have joint capsular tightness, these mobilization techniques may help to improve ROM and pain. I like how Kelly encourages the person to take an active role in their rehabilitation rather than fall into a therapist dependent passive treatment. However, If you have persistent or chronic pain, which is the problem, these more than likely offer only temporary relief because you haven’t addressed the sensitized nervous system. Mind you, these mobilization techniques have been existed for years and haven’t shown to be any more effective in treating persistent pain than other techniques. I would have been happy if the book stayed within the realm of athletic, lifting injuries and proper form, and stayed far away from treatment or prevention of pain.
- Compared to normal weight, overweight has a 6% decrease in mortality. How is that for a surprise?
- The mortality rate for obese was similar to normal weight
- The mortality rate for obese (>35 BMI) was much higher than normal as expected.
- The mortality rate for underweight (<18.5) was much higher than normal as expected.
- The results are strikingly consistent across all ages, gender and population
- My Comment: His criticism was picked by a lot of bloggers and even researchers and just ran with it. If people take 10 minutes to read the study than just blindly following what other prominent people say, this criticism would have never came up. From the original article, “The results presented herein provide little support for the suggestion that smoking and preexisting illness are important causes of bias. Most studies that addressed the issue found that adjustments or exclusions for these factors had little or no effect.” Basically, it means almost all the studies included in the analysis were adjusted for smoking, age related weight loss, smoking, and illness related weight loss..
- My Comment: This is not one study, but a collection of multiple studies (called meta-analysis)These results are only controversial, if you are unaware of the literature. These results are consistent with previous studies. For example, the same author published a meta-analysis in 2005 showing no increase in mortality in overweight people (2). This was repeatedly shown in other meta-analysis done by other authors too (3,4) . It is now pretty much established that in the presence of chronic conditions like heart disease or diabetes or older age, being overweight or slightly obese can be protective or the excess body weight makes them live longer. We even have a name for it called the ‘obesity paradox’.
- My comment: This is a valid point but is not a criticism of the study per se. The study aim was to look at mortality and not morbidity. It is true that as BMI increases there is an increase in disability, medication, health care costs, and unhealthy life years. And they do mention it in the study as a limitation.
- My Comment: The author is Katherine Flegal and works for the health statistics department at CDC (Center for Disease Control & Prevention). These people have the best bio statisticians in the country.What most people are unaware is that, she is the very same author who publishes all the ‘good’ news about the obesity prevalence in America. If there is any researcher in this world, who wants to see mortality goes up with BMI, I reckon it might be here since she is the one who showed/showing us how America is getting fatter.
On a personal note, she is one of those fantastic researchers that everyone can look upto. Even when she was pummelled with personal criticisms (and this dates back to 2005), she has responded very professionally everytime and left out the personal attacks and remarks that could have easily been justified. He letter responding to article comments in JAMA is just a beautiful example of how to respond to criticisms. I personally wrote a thank you letter which she gracefully replied and forwarded to her co-authors. In fact, the prestigious science journal Nature wrote an extraordinary editorial literally scolding Dr.Walter Willet for taking his criticisms too far against fellow researchers who don’t agree with his conclusions. - Deaths from obesity or being fat is mainly due to heart disease. But now with all the new prescription drugs available for blood pressure and cholesterol, there is a dramatic decrease in heart disease deaths. It has been shown that the levels of risk factors are now way lower than that of lean individuals 20-30 years ago. Further, it is been known that obese and overweight people are more likely to visit doctors, be screened for disease and be treated compared to lean folks.
- BMI is not an accurate indicator of body fat or the location of body fat. People with normal BMI can also have body fat percentage consistent with obese folks. Likewise, folks with higher BMI can have body fat levels comparable to a normal BMI individual. It is also now known that the location of body fat plays an important role in predicting health risks; abdominal fat posing the greater health risks This is why waist circumference is usually recommended as an additional marker among with BMI for health risks associated with excess body fat. BMI is also not an accurate indicator of the presence or absence of risk factors like cholesterol, blood pressure. and diabetes (8).
- Cardio respiratory fitness has now been shown to be an independent predictor of mortality. Studies have shown mortality risk of people who are fat, but fit to be twice lower than lean, but unfit folks. So you can be fat and still be fit and healthy, and live longer. This is the popular fit vs fat concept by Dr. Steven blair.
- As mentioned previously, presence of chronic conditions like heart disease or diabetes or older age, being overweight or slightly obese can be protective. This could be due toThe optimal BMI for people with chronic disease could be within overweight and obese level (5). As shown in this study, this maybe true for the population without any chronic disease, but needs to be further investigated.
- BMI is just one risk factor and a minor one in the assessment of health risk factors. BMI should not be used as a sole determinant for health risk assessment. If you are overweight or obese (less than 35) you need to look at other risk factors such as waist circumference, cardiovascular fitness, blood profile (cholesterol, blood pressure,..) before you start panicking about your weight.
- Although, there is no increase in mortality with being overweight or obese (<35) BMI, there is an increase in morbidity or sickness with BMI ( decline in function, disease,long-term medication, medical costs and so forth). So your quality of life or health is better if you can stay around normal weight.
- As Dr. Flegal, the author of the study, puts it: We are absolutely not recommending people overeat. We intended our research to give a little perspective – to counter the view that if you weigh a bit less you will live forever or if you weigh more you are doomed. The relationship between fat and mortality is more complicated than we tend to think.
- Muscle memory phenomenon can be largely explained by muscles maintaining their muscle nuclei during muscle loss or detraining.
- These results are yet to be replicated in human studies.
- Power training seems to be slightly better than regular strength training in older folks to improve physical functioning
- The only simple modification required to do power training is to lift the weight as fast as possible.
- This is a very important area of research and has lot of unanswered questions, and more research is clearly needed
- Next time when you train an older client or if you are old and working out, keep this in mind.
- Basic science studies: These studies looks at the science behind treatments/drugs/ and try to expand our basic knowledge. For example, how does occlusion works in increasing muscle, how does stretch affect protein synthesis and so forth.
- Applied research: These are basically studies which look to see if a treatment or drug works or look at practical questions. We don’t care what is the mechanism behind it or if we learn anything new.
- You had clients who are genetically gifted
- You had clients who were really motivated. We know how much your diet and lifestyle can influence how you look.
- You had a clients who were beginners or in their developmental stage
- You clients just happened to be on a really crappy program and/or diet before they came to you
- You are just consciously or unconsciously ignoring clients who left or didn’t get results and counting just the positive hits
- Evidence-based approach evolved not to understand the mechanisms or explain the why, but to get results
- Evidence based approach primarily uses applied research and less of basic science research
- Your results says very little about your program or you as a trainer. Most good trainers know this .
- Unfortunately, we do not know what magnitude of compressive forces (patellofemoral and tibiofemoral) can be damaging to the menisci and cartilage.
- Unlike the ligaments, menisci and cartilage do not get stronger and thicker with repetitive loading. They just wear off and cause patellofemoral degeneration and pathologies, such as patella chondromalacia and osteoarthritis.
- We know the patelleofemoral and tibiofemoral forces are at the highest during deep squats. What is uncertain is if these forces will actually cause cartilage/menisci damage and end up showing as knee pain. This will depend on a lot of other factors such as genetics, the weight you use, how often you squat, age and so forth.
- Considering how pain is extremely complex and is not linearly related to damage, the issue becomes all the more complex.
- If you are an olympic lifter, you have no choice but to deep squat. If you are a bodybuilder, it might be better to deep squat to target your glutes. If you are a lay person who wants to look good and love having some heavy weight on your shoulders, there is no compelling reason for you to do deep squats. If you are a 50 year old with some nagging knee pains, it may be better to avoid deep squats
- To sum it up, there is no conclusive evidence to show deep squats are either safe or unsafe for your knees.
- Contrary to what most people think, research will rarely give a definite yes or no answer that we all love;there is always some uncertainty. Our job as evidence-based practioners, instead of ignoring or disregarding the uncertainty, is to accept the uncertainty and convey it truthfully.
- Subjects: Eleven healthy male who had moderate resistance training experience (moderate to very active).
- Design: It was a within subject design. That is, one leg served as the control and the other leg as the experimental group.
- Protocol: The protocol involved rolling their quads for 2 minutes with a 30 sec break. So the subjects rolled out their quads 3-4 times during each minute
- Outcome measures: The outcome measured were flexibility or ROM of the quads and force changes.
- Results: The study showed a 10 degree increase in ROM after foam rolling compared to the control leg. Yahoo! Also, there was no increase or decrease in the force measurements after foam rolling.
- Not blinded: Ideally, the control group should have received a similar treatment or sham treatment which feels or looks like foam rolling, but doesn’t have any of the benefits of foam rolling. It is just like giving a sugar pill to the control group in a drug trial. The reason we do this is people would see an increase in performance just by believing that they are doing something that is beneficial. This not sometimes practical, especially when the subject has their same leg as control. That been said, the validity of such studies are always low.
- Passive control: The control group did nothing here. It is now known that drug-industry funded trials show large treatment benefits compared to non-profit funded studies. And one major explanation for this is using a poor control group. The industry funded trials purposely pick a placebo or a sugar pill as the control when they could have used an effective drug or use a low dose of the control drug just to make their drug look great. It is like comparing P90X program to a control group who just sat on their butt and then saying P90X works great in increasing muscle!
- Reliability: Reliability simply means consistency. It is critical that the test we use to measure our results give us the same readings when the test is repeated. Validity means whether the test is measuring what it is supposed to measure, in this case the knee ROM
- Normally, the Ely’s test is used for measuring the knee ROM. But the authors had to use a modified version since the subjects were more flexible than normal. In a recent study, the Ely’s test was shown to be lacking reliability. In fact, the study used experienced clinicians and still the flexibility measurements ranged as much as 20 degrees (the difference in this study was 10 degrees). And this was for an accepted standard test. Now imagine the reliability & validity of a modified test which the authors came up with without any pilot study data?
- Unblinded outcome assessors: In any study, it is quite easy for the study staff to consciously (or unconsciously) read or manipulate the numbers a bit high or low when they know the treatment group. So it is very important to use people to measure outcomes who are unaware (or blinded) of who belongs to which group.Here they were not blinded.
- In a recent meta -analysis, it was shown that that studies that used unblinded outcome assesors showed larger strength gains compared to studies which used blinded outcome assessors. Now it is not very hard to imagine how crucial blinding becomes when the measurements are highly subjective as in this study. Here the assessors ‘pulled’ the leg till the subjects had to say otherwise.
- Surrogate measures: I have wrote about this in the past. The study uses surrogate outcomes like static flexibility and ROM which means nothing to an athlete. I would be more interested if they tested the vertical jump or the squat or other outcomes which are meaningful to an athlete or a weight trainer. Increase in static flexibility has not shown to improve performance nor prevent injuries.
- Looking at the above factors, the applicability of the study is pretty minimal. I wouldn’t start anyone on foam rolling based on this study. One positive aspect is the study showed no force decrements with foam rolling. This is a major concern with foam rolling when it is theorized to work by activating an inhibitory response in the muscle. These inhibitor responses are not what we want before training for a race or lifting.
- For people who have the time and who love foam rolling, you can keep doing it. Instead of bashing research, just say “we don’t have any studies to show it doesn’t work and my clients are getting results. This is my anecdotal evidence and I maybe wrong”.
- But for people who don’t have the time, nor care about how they feel, a dynamic warm up (which is more active, gets the blood moving, and more functional) is the better option. Foam rolling ,on the other hand, cannot serve as a warm up and it is completely non-functional.
- Blood letting: Blood letting (letting blood by cutting your vein) was the major medical treatment for almost 2500 years. It was considered as a major treatment when it was killing more people than it cured. And you know why? It was because the doctors were getting ‘results’! If we couldn’t see people dying in thousands, tell me how we are going to see a 10 degree difference or performance improvements in the range of milliseconds?
- Smoking: Smoking is now universally considered to be hazardous for your health. But this realization only came after much careful research in the 1940’s and 50’s. People were dying or the ‘results’ were for us to see, but we had no clue until the research showed it. And why is this? This is because of the random variability. Some heavy smokers died young, while some lived to their 80’s and 90’s. The same variability exists with any intervention whether it is weight training, smoking, or foam rolling. The only way to minimize the variability and get the true picture is through systematic observation and not by more anecdotal ‘results’.
- Lean Body Mass: Lean body mass consists of muscle, bone and water. So an increase in water content will also show an increase in lean body mass. But this increase in LBM was hwon to be mainly due to extracellular water and not actual muscle fiber.
- Collagen: GH also increases lean body mass by increasing collagen in muscle and tendon. Collagen is mainly found in outer covering of muscles (connective tissue), tendons and skin.
- Strength: GH has also shown no increase in strength or power in healthy adults
- Growth hormone supplements do not work to increase muscle or strength or for bodybuilding
- Growth hormone supplements also has some pretty serious side effects
- Case closed.
- Testosterone supplement tribulus do not increase testosterone or testosterone precursors in humans
- Tribulus do not increase muscle, decrease body fat or increase strength
- Tribulus terrestis works if you are a rabbit or a rat
- Enter your current weight, height, age and activity level
- Enter your desired weight & duration you need to lose this weight
- Enter the increase in physical activity
- You will get the calories you should eat to reach this weight and the calories required to maintain this weight.
- There are a lot more features in the results, like body fatness, results in tabular form and so forth.
- There is a 5% error in calculating the basal energy requirements
- The adherence is assumed to be perfect
- Changes in energy intake which can effect changes in energy expenditure. For example, people eating more after they work out
- There are genetic factors which can change the weight lost or gained.
- The old equation is static and clearly overestimates the predicted weight loss
- The new equation takes into account the loss in muscle mass and the drop in calorie expenditure with weight loss
- Though it has limitations, the new equation can predict the calories required or activity needed to lose a certain amount of weight in a certain duration with a greater accuracy than it has ever been possible.
- Though you will increase amino acid levels in the blood, you will not increase protein synthesis or maintain protein synthesis levels by eating protein every 2-3 hours.
- A better strategy would be to space protein every 4-5 hours. We don’t have any long term studies to confirm this hypothesis.
- Also for most people, eating protein every 4-6 hours would be lot easier than worrying about getting protein every 2-3 hours every day.
- Try it out for a few weeks. If you don’t see a decrease in strength/muscle or see an increase in strength/muscle, stick with this strategy.
- Obese people will set realistic goals (5-7%). Most people set weight loss goals looking at magazines or they think they have to come down to normal BMI to be called 'healthy'. If it can be maintained without extreme difficulty, try to lose more.
- People will immediately focus more on weight maintenance than weight loss. I always tell my clients that “weight loss is easy, weight maintenance is the hardest part”. People just don’t get this idea because they have no clue about the biological basis of obesity whatsoever. People will think long term, and will think more about how to maintain their weight loss than how fast they can lose the most amount of weight. The typical Before-After picture is an example of weight loss - not weight maintanance.
- People will finally stop looking for the perfect diet or bothering incessantly about whether it is fructose, crabs, fat and so forth. They will finally stop blaming their diet for failing them. There will be less tress wasted on diet books.
- Normal weight and lean people would look at obese from a different perspective - one filled with compassion and empathy.
- And for the most important part: Obese people will finally understand that it was never their fault. They will finally be free of their endless self-blaming, depression, and lack of self-esteem that they had to endure their ther whole life.
- And this world would be a much better place to live in.
- Exercising and eating healthy have a lot of benefits independent of weight loss.
- Lose 10-15 lbs (5-7%) of your weight. There are a lot of health benefits of losing such a small weight. This is what even the research recommends.
- If you can maintain this loss without gong crazy, you can always try to lose more. At least now you know what you are dealing with.
- Unlike what most people think , environment - whether fructose, carbs, portion size, low activity, or whatever- only causes a modest weight gain in the majority. But when converted to obesity prevalence, this modest number turns into large percentage increases. This gives the wrong impression that everyone is putting a lot of weight.
- Like it or not, genetics play the largest role in obesity.
- There is no other populaton that has suffered such discrmination and bias for all these years, even in this 21st century. All this because of our casual beliefs based on some personal experiences and observations that obesity is largely determnd by lifestyle/environment and lack of willpower or everything except genes. I think it's time that we showed more compassion to these people whose only fault is that they ate because they were hungry - just like me and you.
- Leptin: The discovery of Leptin is one of the greatest discoveries in the field of nutrition. Leptin is primarily secreted from fat. When you lose weight, leptin levels goes down and signals the hypothalamus to increase appetite and decrease metabolic rate. When you gain weight, leptin levels increase and in turn suppresses appetite. The picture shows leptin defiency treated with leptin administration.
- Ghrelin: Ghrelin is another hormone secreted mainly from the stomach. Ghrelin is a short term modulator of hunger; food intake decreases ghrelin, while starvation increases ghrelin.
- There are other hormones like CCK, choleskylin, amylin and so forth that are part of a complicated network evolved to maintain the homeostatic control over your body weight.
- Other Genes: Mutations of other genes involved in energy balance has also shown to cause massive obesity. Leptin receptors are located in the hypothalamus and lesions in these areas have shown to cause massive obesity and thinness in both animals and humans.
- Children: There is a growing body of studies that show a positive relationship between exercise and cognition and children. Exercise has shown to have a positive relation to cognition in 8 cognitive measurement categories (math test, verbal test, memory, academic readiness, perceptual skills, IQ and achievement) except for memory for all age groups.
- Exercise has also shown to improve academic performance. A few studies have shown no change in academic performance with exercise. But none of the studies have shown a decline in academic performance by increasing the time allotted to exercise. The below graph shows a significant improvement in academic scores with exercise in elementary school children after 3 years compared to a control group. This is ironical considering physcial education is the first to be cut from the curriculum owing to financial constraints.
- Older Adults: Now there is an overwhelming number of studies to show that exercise is important for maintaining brain functions with age and also in lowering risk for cognitive decline and dementia.The greatest improvement is seen with executive cognition function which involves tasks such as planning, scheduling, inhibition, and working memory. In fact, executive cognitive processes suffer the most with ageing (5,6,7).
- Surprisingly, with just 35 sec rest, circuit training group had similar power, strength increase compared to the traditional training group.
- There was an a decrease in body fat and an increase in body fat in both groups. The decrease in body fat was only significant in the circuit training group though.
- Both groups improved in aerobic and anaerobic tests
- Circuit training with heavier loads can increase strength and muscle similar to traditional routines.
- Circuit training can cut your workout time by almost half.
- Power balance band or power balance bracelet do not work. Period.
- If you still wear it, you are just openly endorsing your lack of basic critical thinking skills than anything else.
- Dis-regulating energy systems : Cancer cells come up with their own energy systems to sustain their uncontrolled growth and proliferation.
- Avoiding immune destruction: It is assumed that many potential cancer cells are destroyed by the immune system, but many cancer cells know how to hide from such immune surveillance.
- Participating in sports may help you become better at real life activities which require multitasking and greater processing speed.
- The study however do not exactly answer the question if these cognitive differences are due to adaptation to training , practice, or just simply better genetics that predispose them to be athletes.
- A neat little study would be to take inactive people, make them participate in a sport, and test if they improve in everyday tasks compared to a control group.
- There is no difference between the drugs. Or nothing important is happening. This is called the null hypothesis.
- There is a difference between the drugs. Or there is something important happening here. This is called the alternative hypothesis.
- The first is the null hypothesis or the default hypothesis that Casey Anthony is not guilty.
- The alternate hypothesis is that Casey is guilty.
- Cheap & quick: These surrogate measures only need a small sample size and are relatively short-term studies. For example, to study mortality you will need a study with 100’s of participants for a period 5-10 years.
- Preliminary: Most studies use these designs as preliminary evidence to justify long-term studies with meaningful outcomes.
- The outcome measure is the most important aspect of a study. Next time, when you read a study or hear someone quoting a study, look to see if it is a surrogate measure or not.
- If it is a surrogate measure, be skeptical about the conclusions.
- If you know about other surrogate measures used to prove a hypothesis, please comment below
- The wide grip pulldowns to the chest showed the greatest activity for the lattisimus dorsi compared to wide grip pull downs behind the neck, closed grip pull-downs (V grip), or a supinated grip.
- A recent study (2010) concluded that that the width do not really matter, what matters is the wrist position (pronated or supinated). A pronated wrist position ,irrespective of the width, is optimal for maximally activating the lats
- A comfortable grip width for lat pull downs ,with pronated wrists, pulled to the front is the best position for lat pulldowns
- Focus on your diet, weight progression and sleep. These are the top things which will make the biggest difference in your physique.
- Anytime you start to worry about certain aspects of your workout, ask how big of a difference will it make in your physique?
- Nine untrained men performed four single joint biceps exercise per week for 11 weeks.
- For two training sessions, 3 leg exercises(leg press, leg extensions and leg curls) were performed before the bicep exercises for one of the arms (hormone Group).
- For the other two training sessions, the same protocol was performed for the other arm without the leg exercise (NO hormone group)
- This type of within-subject design ensures that motivation levels and genetics do not affect the results.
- Both group increased muscle CSA, 1RM strength, peak power and muscle volume.
- Only the hormone group obtained significant increase in muscle CSA at the part of the arm with ht e largest cross sectional area.
- Only the hormone group showed a significant improvement in 1RM strength in biceps
- One of my concerns is the design of the study. The design of having them do leg exercises before arm exercises is not ideal. The acute increase in catecholamine and the neural drive after leg exercises makes you feel stronger which can be evident especially in smaller muscle exercises.
- The % strength increase for the no hormone group is 14% (12lbs) and 21% (18lbs) for the hormone group. In the previous study, they saw a 24% increase in strength for the no hormone group and they did only 3-4 sets compared to 6 sets in this study. That is almost twice more than what they got here!
- Though the results are statistically significant, the difference of only 5-6 lbs in 11 weeks in beginners is not really impressive.
- The muscle cross sectional area (CSA) increase was significant in all sections for both the groups except section 8 & 9 (circled in red in the figure) for the no hormone group. But the author for some reason only mentions the significant increase in section 8 of the hormone group in the abstract. In the previous study, all sections in both groups had a significant increase in CSA.
- The CSA increased more in one group, but the muscle volume inexplicably remained the same for both groups.
- Even after doing 6 sets of biceps exercise after leg exercise for 11 weeks, the increase in biceps strength was only 5-6 lbs in rank beginners in the hormone group. Hence the benefits of such a training protocol for trained individuals is dubious.
- Based on this study, performing just leg exercises and increasing hormones will not make your biceps grow. You have to perform sets of bicep exercises and make sure they are done ‘right’ after the leg exercises.
- Considering that this is the only study which gives a causative role for the hormone theory, the evidence is still weak for a theory which is still the most popular theory of muscle growth.
- The point is you will only feel pain when the brain feels it indeed dangerous and you need to be protected.
- This happens at the unconscious level and you cannot control what your brain is thinking in that split second. What your brain thinks depends on your combined input of previous beliefs, social context, attitudes, expectation, sensory cues and such
- So the goal of any pain treatment should be to lower the threat level in your brain. One way to do this is to understand the physiology of pain and the fact that ‘pain is in your brain’.
- Be in that obese category where you are 100-200 lbs heavier. The heavier you are, the greater the weight loss
- You are ready to quit your job, leave your family and move to a ranch with only one goal in mind.
- You have enough money to hire a trainer to train you everyday and keep you accountable.
- You know millions of people all over the world are watching you on television and judging you on how well you do. How is that for accountability?
- You have thousands of dollars to look forward for achieving your goal.
- Lose 5-10% of your weight and try to maintain for 6 months. If you can maintain it, go for more.
- Even losing 10 percent of your total body weight can have significant improvements in blood pressure, blood cholesterol, and blood sugars.
- When you think of making dramatic changes to exercise and diet, ask yourself if it is healthy and if you can maintain it for the rest of your life.
- The Biggest Loser show is inspiring, but clearly has nothing to teach you about healthy weight loss and weight maintenance.
- There may not exist a direct relationship between performance and the cellular events measured. So increase in AMPK may not mean a thing when it comes to increasing performance.
- Muscle function is just one factor in determining performance. Performance might be dictated by an integration of several factors such as the nervous system, mechanical efficiency and such
- We lack the tools sensitive enough to detect small increments in performance.
- Training with low glycogen can have negative effects on training intensity and the health of the athlete which might compensate for the positive effects of low glycogen training
- Finally, there might be some complex combination of training and nutrition which we haven’t nailed it yet.
- There is no clear advantage of training with low glycogen levels on performance measures, atleast from the current studies
- Elite athletes already might be training with low glycogen levels due to practical reasons. Sessions done after overnight fasting, with low carbohydrate levels, twice a week sessions can stimulate low glycogen training.
- If low glycogen training is attempted it is better to do it early and away from your competition period.
- The results showed that no-MRI groups came off disability around 200% faster than the low-propensity early MRI subgroup!
- Medical costs were also dramatically different and in the same direction.
- The risk of having surgery for the no-MRI groups was reduced to 3% and 10% in comparison with the early MRI group (100%).
- Detox or cleansing diet cannot clear toxins or chemicals from your body as claimed. The short term benefits has nothing to do with toxins removal.
- We already have an inbuilt detox system in our body namely kidneys and liver.
- If anything is removed with the detox diets, it is your money from your wallet.
- Retrospective: The study is looking comparing 2 groups . The first group trained in 2004 while the second group trained in 2005. The author looks back at these numbers in 2010. Retrospective studies usually cannot make cause and effect conclusions because there are so many variables that are not controlled.
- Volume and Intensity: The volume and intensity was not equalized and hence says nothing about the autoregulation/periodization.
- Pre-test and Post Test: The pre-test numbers are in fact the post test numbers after the off season. So the numbers might have gone up or gone down in that break period.
- Results: The is a bit sketchy. The results are given in N when the training weights and such given in lbs. The results how that the Autoregulatory group went up by 90 N (20 lbs) in bench while the squat by almost 180 N(40lbs). The bench press periodization group had no increase!
- Beginners: In beginners, it is better to stick with traditional sets and reps. You need few years of training before you can really go by feel. Also, if they go by instincts, most beginners will rather sit at home and watch TV.
- Advanced: Most advanced lifters use a mix of planned and auto-regulated type of training. They will have a basic template of the sets, exercises and which weeks to go hard and light. The weights, sets and reps will change based on how they feel that day. Some call it cybernetic periodization.
- Length of Training: Autoregulation is best done for periods of 4-6 weeks. In autoregulation, you are training to your maximum weight for that particular rep and hence can easily get overtrained if you don’t have a plan to manage fatigue. And I think the duration of the cycle can be partly attributed to the results of the above studies.
- Vasodilator: Nitric oxide works as a vasodilator. It means it dilates or expands, especially tubes through which blood flow (blood vessels).
- Arginine: Arginine is an amino acid and produces nitric oxide (NO) in the body, so the supplements which contain L-arginine are essentially nitric oxide supplements.
- Increased Blood Flow: Since nitric oxide expands blood vessels, it is claimes to increase blood flow and oxygen to the muscles during exercise.
- Increased Protein Synthesis: Increased blood flow means increased transport of amino acids and nutrients and thereby greater protein synthesis and muscle growth.
- Clinical Population: Number of studies have shown that In conditions where NO production is reduced (common in various conditions such as cardiovascular disease diabetes, hypertension, etc.), arginine supplementation can increase NO production and blood flow.
- Healthy Individuals: In healthy individuals, who have normal NO production, oral arginine supplementation do not further increase nitric oxide and thereby blood flow. This was shown in number of studies.
- In healthy individuals infusion of very high doses of arginine (3-4 times higher than oral dosage) has shown to increase NO and blood flow though.
- Protein Synthesis: This was also tested in a recent study in healthy individuals. They found 10 gms of arginine supplements taken before resistance training neither enhances blood flow nor protein synthesis compared to a placebo without exercise.
- If you have cardiovascular diseases, diabetes, burn injury and such, nitric oxide supplementation can increase blood flow.
- For healthy individuals , Nitric oxide supplements do not increase blood flow to the muscle or protein synthesis as claimed by NO supplements
- Body fat: You cannot burn body fat from specific areas of your body by exercising those specific areas. This is called the myth of spot reduction. It is the same reason why millions of Americans who does thousands of crunches at the gym still have no abs. So shake weight fails big time for fat loss.
- What about the calories burned? You might burn 30-50 calories with a 6 minute workout since it only uses small muscles groups, with a small range of motion, and for very short time. To burn a pound of fat, you need to burn 3500 calories!
- Muscle Gain: There might be some increase in muscle in your upper body for a beginner for the first few workouts, but then your muscles adapt. Since there is no progression in weights with a shake weight, which is the cardinal rule of muscle gain, no shaking will ever get your more muscular.
- Tone: You look toned when you lose fat and gain some muscle. Since shake weight fails to do both, guess how can it make you toned?
- Pump: Most of the shake weight ads show people using it and feeling the burn in your arms and upper body and they think “wow it works”. You can get a regular dumbell and shake it too and you will feel the same. Or get a bottle, fill it half way, and shake it .
- Harm: It is now well established that vibration exposure can cause harmful effects. According to OSHA (Occupational & Safety Hazard Association), long term exposure to vibration can also cause nausea, impaired vision, hyperventilation, and disorders such as White Finger Disease (Raynaud’s Syndrome), Hand-Arm Vibration Syndrome, & Carpal Tunnel Syndrome.
- Shake Weight do not work to get toned, gain strength, muscle or burn calories.
- Regular use of shake weight may cause some vibration exposure problems.
- If shake weight helps anything, it teaches you how to market the wrong product the right way.
- For high impact sport athletes, FMS can be a worth while screen though this is not as black and white as most see it.
- For the lay people or the average joe who goes to gym, FMS cannot be justified as screen
- What I wrote above is an integral part of evidence-based approach, which is not all about research studies as most people think.
- Drug A can lower the risk of dying from cancer by 25%
- Drug B can lower the risk of dying from cancer by 0.1%
- Drug A (25% reduction) is expressed as Relative Risk
- Drug B (0.1% reduction) is expressed as Absolute risk
- Drug Company: A drug company will always write risk reduction in relative risk to make the benefits look great and the side effects in absolute risks. So you might read an article that Drug A will lower the risk of deaths by 25% and the risks of developing side effects is 1%. That is great drug you will think!
- Caring Doctor: A caring doctor will usually express the risk in absolute terms and avoid percentages. So if the risk is .1% , he will say we will have to treat 1000 people with this drug to prevent one death(shown in the pic). This concept is called Numbers Needed to Treat (NNT).That is not that great as you previously thought!
- Risk/chance can be expressed in relative risk or absolute risk.
- Relative risk is always higher than absolute risks and hence often misread.
- It is better to use absolute risk or the Numbers Needed to Treat (NNT) concept to get the true picture.
- Every time someone asks if a new program or diet or drug works, ask if it works for what, who, and compared to what
- When you read a study, look what are they measuring, in whom they are measuring and what are they comparing it too.
- Happy New Year!
- Soreness is not a reliable indicator of muscle growth and soreness is clearly not required for muscle growth.
- Soreness only means you have caused muscle damage which may or may not result in muscle growth.
- 9 recreationally active subjects were randomly assigned to a Protein only group and a protein + carbs group.
- Participants performed 2 trials seperated by 7 days of 4 sets of leg extensions (8-12) for failure after an overnight fast.
- The protein group consumed 25 gms of whey protein while the protein+carbs group consumed the protein with 50 gms of malto dextrin
- As predicted, the glucose and insulin levels was significantly greater for the protein+carbs group
- But, guess what, there was no difference in protein synthesis or protein breakdown between the protein only group and the protein plus carbs group.
- There is no reason to add carbs in your post workout shake to decrease protein breakdown or increase protein synthesis.
- The protein itself in the shake is enough to increase insulin levels and decrease protein breakdown to the maximum extent
- Strength is very specific to the repetition range.. There is no magic to low reps that is missing in high reps in increasing strength
- If you are training for muscle, there is no reason to add low reps to increase “strength” as most people say.
- Straight leg exercises target both the soleus and gastroc muscles. Seated calf raises only target the soleus muscle.
- Straight knee stretches target the gastroc muscle while bent knee stretches target the soleus
- Common cold is the major cause of visits to the doc in western countries and absentism from work and school
- Worse yet, you to miss your workouts too!
- Anitbiotics are ineffective since common colds are caused by viruses
- Vitamin c has been widely sold to treat and prevent common cold
- High quality methodology: Studies were accessed for blinding, random allocation , placebo indistinguishabilty, allocation concealment, studiy search done by independent authors and sought intrepretation only when data is questionable.
- Treatment: Orally administered vitamin C of at least 0.2 g daily for a single day or for a period.
- Outcome: Outcome measures were incidence, duration or severity of the common cold.
- Prevention (incidence of colds): There is very little benefit of taking vitamin C routinely to prevent colds. In special circumstances, If you physically very active and /or exposed to cold conditions (marathon running, skiers), vitamin C could beneficial to prevent colds. This was consistently shown even with smaller doses.
- Treatments after the onset (therapeutic): No trials have shown it to be effective. But since vitamin C has consistently shown to decrease the severity and duration, it might be worth a try. We need more studies to see if high doses ( 8g/day) can have a therapeutic effect and if supplementation is more effective in children than adults.
- Dosage: The effective dosage can be from 1 gms to 8 gms.
- If you live in cold countries and is highly active or prone to colds (athelete or heavy lifting, dieting), supplementing vitamin C during the winter could be beneficial. The dosage could be from 1- 4 gms.
- There is little practical benefit of taking it year round.
- If you already got a cold, try some high doses as soon as you can (4g - 8g). If it doesn’t work, have some chicken soup instead
- Science of training: This part is the crux of an evidence- based approach and is called the “science of training”. The best evidence is obtained from high quality randomized experimental trials to determine the effectiveness of a particular workout program/supplement/diet and so on.
- Example: For example it is clear from reviews and meta-analysis that multi-sets are better than single sets to increase strength and muscle in intermediate and advanced lifters. It is clear from studies that supplementing creatine with your workouts helps with muscle growth and strength.
- Art of training: No evidence can replace the trainer’s/coach’s expertise and experience. This is what they call the “art of coaching or training”.You will never find a study where the subjects are exactly the same as your clients. Ironically , the number one criticism against the evidence based approach is that evidence based approach ignores trainer’s/coach’s expertise and judgment and is just a cookie-cutter approach.
- The client’s age, training history, injury problems, biomechanical constraints, fitness assessments , stress level, personality , sleep, diet, genetics, skill can all have an influence on the effectiveness of the workout program and hence the evidence needs to be tailored to the individual client.
- Example: For example, an older client with stressful job will need much lower volume to maximize recovery. Also, the evaluation and correction of the exercise technique is solely dependent on the trainer’s experience and expertise
- Client, client, & client: The client goals and preferences are important though the best evidence may not recommend this option . For example, taking long rest periods in between low reps when the client don’t want to sit around and waste time. Though the best evidence shows that long rest periods are optimal for low reps, this may not be the optimal decision strategy for that particular client.
- Example: I have come across numerous times when trainer makes the client do a lot of funky functional exercises on the ball when the client just wanted to lose weight. This is where the trainer’s preference is taking precedence over the clients preferences
- They can produce more force than concentrics. So you can use more weight than concentrics.
- They selectively recruit Fast fibers. Fast fibers are bigger and have greater potential for growth than slow fibers
- They recruit less fibers than concentrics and hence accumulate greater damage and greater protein synthesis ( and greater protein breakdown too , mind you).
- The use very little energy and hence has very little metabolic fatigue
- In contrast to concentric, higher velocity generates greater force in eccentrics.
- Meta-analysis: The study combines all the studies comparing eccentric exercise to concentric exercise into one big study.
- High Quality: As like any quality meta-analysis, the study had an inclusion and exclusion criteria, quality assessment of studies by independent reviewers, subgroup analysis based on contraction mode and speed of contraction and so on.
- Included studies: After reviewing 66 studies, only 20 studies were included based on the inclusion and exclusion criteria.
- Strength: Eccentric training is more effective at increasing eccentric strength than concentric training. The greater strength increase was only shown with higher eccentric intensity. But even training with higher eccentric intensity did not increase concentric strength.
- Muscle: Eccentric training appears to be more effective at increasing muscle mass than concentric training. This increase was shown with both higher and comparable eccentric intensities. Some of the conflicting results are speculated to be because of the different methods of measurements used.
- Velocity-Specific: Eccentric strength is highly specific to the velocity of training
- Adding a few sets of eccentric sets for the weaker body parts can be helpful. You can also add few weeks of eccentrics at the end of your training cycle too.
- Eccentric for every exercise or bodypart will be extremely fatiguing and will negatively affect your recovery.
- If you are into sport performance, training eccentric contraction at the velocity of the sport will be more helpful in improving eccentric strength
- This is the problem with results/ testimonials. Everyone seem to have results and it is hard to pick one workout/diet over the other based on it.
- Next time when someone talks about results/testimonials, ask them if they ever heard about reporting/outcome bias and send this article to them.
- That’s one more reason to stick with scientific studies.
- Osteoarthritis: Osteoarthritis (OA) is the most common form of arthritis that can affect the hands, hips, shoulders and knees. In OA, the cartilage that protects the ends of the bones breaks down and causes pain and swelling .
- Glucoasmine Basics: Glucoasmine and Chondroitin are the building blocks of your cartilage and hence is believed to make up for the loss of cartilage.
- Dosage: It can come in combination with other supplements (such as chondroitin), or by itself in the form of glucosamine hydrochloride or sulphate. The usual dose recommended on packages is 1500 mg per day or 500 mg three times a day.
- Benefits: The studies have been conflicting. Studies which shows a benefit used small sample size and had methodological flaws.
- No Benefits: Larger studies with sound methodology shows no or small benefits.
- Meta-analysis: It basically combines the results from a number of studies done on the same topic. It is kind of like a study of studies. So 3 studies of with 10, 50, 100 will be one big study of 160 subjects.
- High Quality: All the studies selected were methodologically superior, large scale and blinded which wasn’t the case of previous reviews. Out of 58 studies, only 10 (3803 subjects) made it to the analysis based on the inclusion criteria. Each study had to have atleast 200 patients.
- Outcomes: The study looked at pain and joint space width (smaller joint space means more cartilage build up).
- Chondroitin, glucosamine, and their combination do not have any beneficial effect on joint pain or on joint space narrowing. Or just basically they don’t work for joint pain due to osteoarthritis.
- The supplement is not harmful and hence people who get some benefits can keep taking it if they have the money.
- The industry-sponsored trials (Rotta brand) showed better results in pain and function than industry-independent trials. Guess why is that?
- These results are consistent with the recent Cochrane Review 2009 on glucosamine and osteoarthritis
- Journal Impact Factor = The number of times an article in a journal is cited in the past 2 years divided by total number of articles published by that journal in past 2 years
- Subject Area: The raking differs a lot based on the subject area. Exercise field’s highest ranked journal has an IF of 4 while basic life science (or fundamental) journals like Nature or Cell has an IF of 40. So comparisons should not be made across subject areas.
- Publication Type: You can easily see that review articles has a lot more citations. Hence journals which only publish review articles will always be rated high.
- Editorials, Letters & Meeting Abstracts: These are included in the numerator but only articles and reviews are included in the denominator. So these letters and editorials can raise the IF of the journal considerably without publishing any major articles.
- Scientific Career: Promotion and tenure in most universities depends on how many of your articles you publish are in high IF journals.
- Librarians: With the price of journals on the rise and so many journals to pick from, librarians need a ranking system bases on objective measures.
- Editors: They need to a objective criteria to see if they are meeting the standards.
- Quality articles: This may not be always true, but the journals with the highest Impact factors are very hard to get accepted in and hence the quality of the articles are always top notch.
- Next time when you are reading an research article (not just exercise journals), it is a good practice to look up the Impact Factor of the journal in which it is published.
- The quality of research articles in journals with high IF is usually pretty high.
- Journal articles should not solely be judged on the journal in which they are published.
- It is not required to train with heavy weights ( less than 5 reps) for muscle growth.
- Using Heavier weights (< 5 reps) can cause greater fatigue, and may delay recovery. Also, there is a risk of injury with heavier weights.
- Moderate weight ( between 5 -15 reps) trained with high intensity is ideal for muscle growth for most folks.
- increase strength & power even in elite athltes
- improve your golf performance
- prevent age-related muscle loss
- increase bone density
- remove toxins and thereby decrease cellulite
- Passive control Group: The control group in the majority of the studies did not exercise. They just sat on their butt. No wonder they saw large improvements in strength and power compared ot the control.
- Improper Control: The studies which concluded that vibration training is as effective as traditional strength training did not normalize intensity. Since the intensity was not normalized, it just could be that the intensity of exercises in both groups were similar and the vibration had nothing to do per se in the improvements.
- Proper control: Now guess what, the studies which employed a proper control where they did similar exercises without vibration saw no statistically significant difference in strength or power.
- Strength and power: None or only minor additional effects on muscle strength and jump performance as compared with performing the same exercises without vibration.
- Speed: No improvements in speed is observed.
- Bone density: There is evidence to show it increase bone mineral density.
- Other: There is no evidence to show that it will remove toxins and decrease cellulite or improve your golf performance or prevent age related muscle loss
- OSHA: It is now well established that vibration exposure can cause harmful effects. According to OSHA (Occupational & Safety Hazard Association), long term exposure to vibration can also cause nausea, impaired vision, hyperventilation, and disorders such as White Finger Disease (Raynaud’s Syndrome), Hand-Arm Vibration Syndrome, & Carpal Tunnel Syndrome.
- There is no conclusive evidence to recommended power plate as a replacement or addition to the resistance training to improve performance.
- Besides increase in bone density, there no evidence to support the claims made by power plate.
- An estimated 310,000 Americans die each year of cardiac arrest. Only about 6 percent of those who are stricken outside a hospital survive.
- CPR allows oxygenated blood to circulate to your vital organs such as the brain and heart and doubles the likelihood of survival for victims of cardiac arrest. Without oxygen, permanent brain damage or death can occur in less than 8 minutes
- Standard CPR: The standard versions of CPR, practiced for more than 50 years, involves cycles of 30 chest compressions and 2 rescue breaths.
- Continuous Chest compression CPR: In the new chest compression CPR adopted by American Heart Association 2 years back, there is no rescue breathing, only chest compressions (100/min)
- People being panicky and being worried about doing CPR wrong were the two top reasons why people don’t attempt CPR.Chest compression CPR procedure is simple to perform and teach and more people are likely to perform it over the standard CPR.( The traditional CPR requires a CPR certification training).
- Most times people do rescue breathing wrong and the breathing the interruption reduces blood flow to the major organs.
- There is no mouth to mouth contact and hence there is no concerns and risks associated with the transmission of infectious diseases
- Chest compression CPR is more effective in certain heart rythms ( ventricular tachycardia or fibrillation).
- No. CPR courses should teach rescue breathing, since it is still preferred in children and adults who suffer cradiac arrest due to respiratory failure by choking, drowning and so on.
- There is certainly a need for rescue breathing after a prolonged period of CPR.We are not sure if we should interrupt compressions for this or not
- Large number of participants: There were 811 participants from diverse backgrounds irrespective of age, income, geography and included a large percentage of men. Obviously the largest RCT related to determine the best weight loss diet.
- High rate of retention: The people who dropped out of the study were low which was a serious problem in other weight loss studies.
- Long Duration: The best weight loss diet study lasted for 2 years which is the longest trial for randomized weight loss trial.
- Compliance accessed: Compliance was assessed by objective markers .For example, urinary nitrogen excretion was used to asses adherence to the protein intake.
- Intense Treatment: Treatment included individual and group instructional sessions to promote adherence.
- 20% fat, 15% protein, and 65% carbs; Low-fat,average-protein
- 20% fat, 25% protein, and 55% carbs; Low-fat, high-protein
- 40% fat, 15% protein, and 45% carbs; High Fat, Average Protein
- 40% fat, 25% protein, and 35% carbs.High Fat High Protein
- Any diet which emphasizes calorie restriction will work and the specific amount of protein, fat or carbs of the diet does not matter.
- Diets should be tailored to the person based on their individual and cultural preferences than based on nutritional recommendations for long term success.
- Behavioral strategies maybe more important in weight loss diets than their composition.
- Intensity: You can put lot more into one set and therefore can use more weight.
- Recovery: If you are doing less sets, you recover better.
- Time under Tension: The time under tension on the muscle is greater and hence greater muscle growth potential.
- Trained Lifters: As you the training age increase, ,muscle becomes resistant to training and hence you need multiple sets to gain muscle.
- Participants: The study had 8 trained participants (atleast one year) .
- Design: The design was within subject design where the subject acted as their own control. This within-subject design minimizes the variables like participant motivation and genetics.
- Training Protocol: The participants after an overnight fast did 3 sets of 70%1RM till failure with 2 min rest in between, and for the other leg they did 1 set of 70% 1RM.
- At 5h: The results showed that both 1 and 3 sets increased protein synthesis at 5 hours, but the increase was significantly higher for 3 sets.
- After a day: Only the 3 sets groups sustained the protein synthesis even after a day while the single set returned back to fasted levels.
- Recent Meta-analysis: The recent meta-analysis confirms with the above acute study and shows that multiple sets are more effective than single sets in building muscle. This was true irrespective of the training status or the training duration.
- Multiple sets are more effective in building muscle than single set.
- 3 sets are more effective in building muscle than one set.6 sets might be more effective that 3 sets, but we are not sure yet
- Are low reps (1-6) better than high reps (8-12) for muscle growth?
- The Best Workout Program For Muscle Growth?
- Shoulder Pain: It has been shown in number of studies that posterior shoulder tightness could be one of the risk factors for shoulder problems and pain.
Weight Lifters: It has been consistently shown in number of studies that overhead athletes, recreational weight lifters and bodybuilders have limited internal rotation or a tight posterior capsule.
The tight posterior capsule in weight lifters could be due the limited internal rotation end-range of motion exercises compared to external rotation exercises.
- If you had to pick just one stretch to prevent shoulder pain and problems, pick the cross body stretch.
- If you have the time, do both.
- The study looked at 12 different trapezius strengthening exercises and they found the below exercises to have the highest activity of LT & MT and lowest activity of UT.
- None of the exercises met the criteria for optimal intermuscular balance restoration of serratus anterior (SA) and LT. Push up and push with aplus are normally prescibed exercises for SA.
- The results of this study suggest that the exercises: A, B, and C are optimal for restoration of UT/LT muscle imbalances. A, B, and D are optimal for restoration of UT/MT muscle imbalances.
- The extreme responders had higher satellite cells to begin with. The authors speculate that your muscle growth potential is partly dependent on the availability of satellite cells before training.
- The satellite cell pool increased a remarkable 117% in the extreme responders during training.
- After training, the Extreme responders had significantly more myonuclei per fiber than Non and Moderate groups .
- The extreme responders in the study are the genetic freaks who can do whatever and still grow like a weed. So don’t think it is their program as most folks do, and copy it blindly.
- As far as I know, the only natural way to increase satellite cells is by creatine. Creatine has shown to increase satellite cells substantially compared to training without creatine.
Related Articles


Should I Take Omega 3 or Fish Oil for Heart Health?
February 04 2022
Omega-3 or fish oils are one of the most popular supplements making over a billion in annual sales. One of the most talked about benefits of omega-3 is for your heart. But are there any benefits? Let’s take a closer look
What do recent trials on Omega-3 & heart health show?
Let’s look at some of the recent trials on Omega-3 and heart health:

For people with/at risk of heart disease:
ASCEND trial (2018):15,480 patients with diabetes but with heart disease received 1 gm of omega 3 or placebo. After 7.4 years, Omega-3 did not reduce the primary cardiovascular endpoints
STRENTH trial (2020): 13K patients with heart disease or high risk of heart disease took 4 g daily of EPA/DHA or corn oil placebo. After 42 months, no difference in heart disease events!
OMEMI trial (2021): 1000 older patients (mean age, 75) with recent myocardial infarction received either EPA/DHA (1.8 g daily) or placebo. At 2 years, there was little difference between the groups!
In the general population:
DO-HEALTH trial (2020): 2200 healthy older adults were randomized both to EPA/DHA (1 g daily) or placebo and to strength training or no training. After 3 yrs., no health benefits were seen
VITAL trial (2021): 25,871 participants, men 50 years of age or older at low risk of heart disease. After 5.3 years, little or no difference in major cardiovascular events.
In short, ALL studies were negative. And mind you, these were very well-designed, million-dollar studies over a long duration of 1-5 years. So, this isn’t the typical 30 subject, 12-week supplement study. I am just amazed how this keeps selling after so many negative trials!
Are there any recent positive omega 3 trials?
Yes. The landmark REDUCE-IT trial in 2018 that had 8K people taking statins who have high triglycerides showed a very impressive 25% reduction in cardiovascular events. But two major caveats:
It appears that the benefit of omega-3 for health is primarily because of EPA and not the combo of EPA + DHA. Also, partially due to the corn oil used in the control group making the omega-3 group look better.
Any recent meta-analysis looking at omega 3 & heart health?
The 2020 Cochrane meta-analysis looked at 86 trials and showed little or no effect for most of the outcomes, such as deaths, cardiovascular deaths, and events and stroke. Omegas may have a small reduction in coronary heart disease events and deaths (coronary means related to the arteries to the heart). These effects did not differ by dosage either.
The table below shows 2 ways to present the number of people that will benefit with omega-3. For instance, for deaths, as shown below if 1000 people take omega-3, there will be 2 less deaths in 4 years. And number needed to treat (NNT) shows 500 people will have to take omega-3 for 4 years to prevent one death!
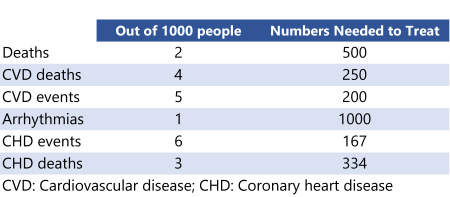
I am a proponent of meta-analysis, but when you meta-analyze studies that have thousands of subjects per study, you run the risk of making tiny effect to become statistically significant. Statistically significant, but practically meaningless.
What about the risk of Omega 3 and atrial fibrillation?
Atrial fibrillation or flutter involves irregular and rapid heartbeat that could lead to strokes and heart complications.
Atrial fibrillation was higher in the omega-3, with higher doses showing a significant risk (STRENGH & REDUCE-IT trial). What is high? For example, STRENTH trial showed a 62% increase with a higher dose of 4gms of EPA plus DHA. This means out of 1000, 9 more will get an AF. Other risks include bleeding and gastrointestinal issues, such as diarrhea.
So, should I take Omega- 3 for heart health?
Related Articles


Can fish oil supplementation cause depression?
January 12 2022
Here is my review of the recent, controversial study in JAMA on fish oil/omega 3 and depression. Remember, fish oil is the most commonly used non-mineral/vitamin supplement in US.
Why did they do the study?

What was the fish oil/omega 3 study design?
What were the results?
What the heck does a 13% increase in depression mean??
Clearly, the individual risk is very low. But this small risk could translate to a big number if millions supplement with fish oils.
Any gender difference in depression?
Women at higher risk: Pre-specified, subgroup analysis showed a higher risk for women, but not men. These were in line with an increase in anhedonia (inability to feel pleasure) and sadness in mood questionnaire items. Keep in mind that these are exploratory and need a further study to be confirmed.

What were the major limitations?
Since we are at it, the parent trial (VITAL) showed Omega-3 and Vitamin D did not reduce cancer nor cardiovascular events - yet another negative study in the long line of disappointing trials on fish oil supplements and CV disease.
What are the recommendations for heart health?
Conclusions
VITAL-DEP Trial (Vitamin D and Omega-3 Trial-Depression Endpoint Prevention)
VITAL (Vitamin D and Omega-3 Trial)
Related Articles



5 Simple Rules for Good Research
December 30 2021
Here are five simple rules for good research from a recent article titled, “Ten simple rules in good research practice for early career researchers”.
An important topic for both researchers and research enthusiasts. Without any further ado, here we go:
1. Register your outcomes & analysis plan:
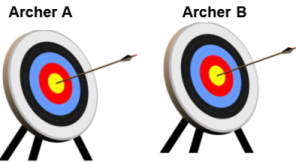
A few caveats:
2. Get statistical expertise
3. Reduce sources of bias
Eliminate biases: When you finally conduct the study, the most important point is to reduce or if possible, eliminate all sources of bias.
Below are some of the most common biases in a randomized controlled trial (RCT’s). In my experience, this is one area that many, including researchers, are either unaware or just ignore. Here is an article that I wrote 6 years back about this issue (How to check the quality of a research article) .
So, the bottom line is if any of these are not controlled for, then your study ends up with “high risk of bias”. Or neither you nor the study author can be ever sure about his or her results! Also, remember these are even important in animal studies. And even pre-registering can’t help you with these biases.
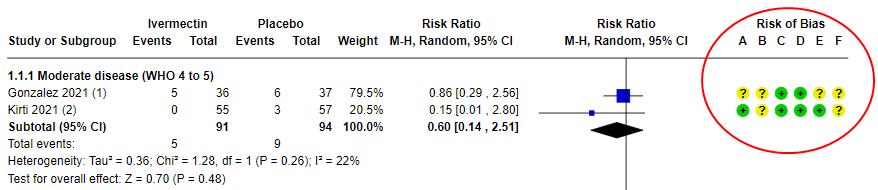
Example: The most cited, recent Cochrane review on Ivermectin concluded that we are uncertain if the drug helps to treat COVID. And guess what? The main reason is that they ended up excluding trials because of ‘high risk of bias’ and was only left with 2 studies. Moreover, the 2 studies that were included still had “some concerns” which ended up downgrading the evidence to ‘very low certainity’ (means we don’t know if it helps or not!).
In summary, a drug that could have saved millions in a pandemic, but we are very uncertain because of the ‘high risk of bias’ in studies. Or a harsher take: People died in these research studies, but their deaths contributed to nothing!! I hope this tells you something about the importance of controlling for biases.
4. Follow reporting guidelines
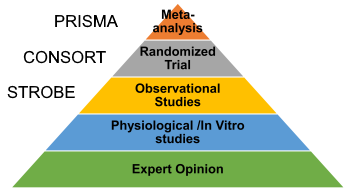
5. Make data open
A good question is if these are so critical, why aren’t these emphasized in research? In my opinion, first is the lack of knowledge on how to implement these: You either have to work with mentors/collaborators who are proficient in these or be very well read or/and up to date in research methodology. And all these takes a lot of time, effort, and even money. Second, there is little incentive for researchers to do these since you are ranked/promoted/hired/judged based on the ‘number’ of publications and not on how well you did those studies. So if you focus on quality, you will be spending lot of time reading and collaborating, which will ultimately stifle your ‘productivity’.
Conclusions

Wishing you all a happy and healthy new year!
Ten simple rules in good research practice for early career researchers
Related Articles
Can we ‘train the brain’ to treat chronic low back pain?
October 19 2021
If you have been following me, you should be familiar with my writings on pain: In 2012, I wrote an article about my low back pain titled "A Revolution in the Understanding of Pain and Treatment of Chronic Pain" which was very popular in the fitness/strength & conditioning community. A year later, I wrote another article - What should fitness professionals understand about pain - further elaborating on these concepts. Ever since I wrote those articles, I was patiently waiting for a major study to actually show that this indeed works.
If you haven't read the articles, here is a very brief summary: In majority of chronic back pain conditions, the pain tissue/injury has healed, but the pain still lingers. Why? The pain is coming from your sensitized nervous system or brain. So the focus should be on lowering this hyper-sensitized nervous system or lowering the threat in your brain.
So what was the study design?
What were the results?
The results were impressive to say the least, and are rarely seen in low back pain treatments.
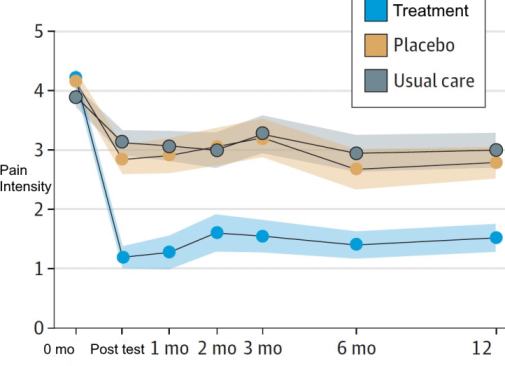
What about previous studies?
A large study published in JAMA in 2018, used a similar model, but the results were negative. The difference could be due to the population (used people with acute back pain), intervention (just 2 hours of pain science education), and comparison group (used patient education than placebo injection). I do think the intervention was more extensive and tailored to the individual in this study.
How is the study quality?
I would rate it as a high-quality study!
- 1. Randomized and allocation was concealed
2. Drop-outs were similar between groups and used an intention-to-treat analysis.
3. No major protocol deviations
4. Outcome assessors were blinded, although not reported in the paper. (I checked with the author)
5. Statistical analysis plan and primary outcome were pre-registered
Any study limitations?
Maybe I am just being picky here or.. :
Which books do you recommend for the layperson?
Explain Pain: An excellent and easy read about the modern pain neuroscience written for people in chornic pain. The Way Out: This book is by the lead author, but I haven't read it.
Conclusion
This is a landmark study with some ground-breaking results that will change the way we look at pain forever.
If you know anyone with chronic back pain, send it to them please.
Reference 1
Reference 2
Related Articles



Generation 100 study - Can higher intensity exercise lower deaths in older adults?
December 25 2020
The benefits of exercise on mortality are largely from observation studies and hence simply associations. The Generation 100 study, published in BMJ, will be the first large randomised clinical trial (RCT) to study effects of supervised, higher-intensity exercise on longevity over a 5-year period.

What was the population?
Older adults living in Trondheim, Norway, aged 70-77 years.
What were the interventions?
Every 6th wk supervised spinning sessions (cycling) with an exercise physiologist were provided with intensity monitored using heart rate monitors. Supervised training with exercise physiologists was also offered twice a week in different outdoor areas. The control group was not supervised.
What were the results?
So why did the study fail?
Was high intensity training really better??
In the abstract, the authors state that they observed “a lower mortality “trend” (non-significant) after HIIT compared with controls (37%) and MICT (49%)”. It means they observed a large reduction in mortality for the HIIT group although it wasn’t statistically significant”. And several leading news channels have reported this study to show HIIT as beneficial.
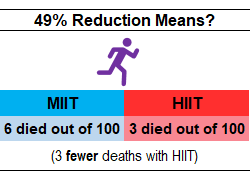
And I have to say this: the article reads like an exercise study in the Introduction, but gradually morphs into a study trying so hard to justify HIT or why HIT wasn’t significant here.
Blah blah… Should I do higher intensity exercise to reduce mortality?
Related Articles



Book Review - Pandora’s Lab: Seven Stories of Science Gone Wrong
October 12 2020
This fascinating book by Dr. Paul Offit illustrates a collection of inventions that according to him had the most impact on the world. Or more aptly, a collection of ‘mistakes’ we made in the past. Dr. Offit is a pediatrician, co-inventor of Rotavirus vaccine, and a prolific science writer.
I am familiar with most of these mistakes (check my article on it here), but there were three (out of seven) that I was least aware of and struck me the most. So here is a synopsis of the 3 chapters:
1. ‘Betterment’ of humans
One of the noblest of goals, but turned out to be the darkest moment in American history- The American Eugenics movement.
Eugenics or “Born well” movement was based on the horrible science that poverty, crime immorality, low intelligence, alcoholism, prostitution, and other mental and social problems are ‘hereditary’. And the best way to make a better nation or human race is to prevent the breeding of these people. The idea originated from Mendel’s pea plant experiments and the selective breeding of animals. Little did they know that humans and animals are incredibly complex than pea plants.
Apparently, bolstered by the bad science, eugenics movement made it to the curriculum in over 350 universities, including the Harvard. Even the immigration ban in US (1920 - 1965) was motivated by the eugenics movement to restrict the “feeble-minded, idiots, mentally or physically impaired or the unfit or the inferiors”. Asians were completely banned and southern and European immigrants were restricted. IQ tests were designed to weed out the “morons” or the “feeble-minded” - people with low intelligence. Almost 60,00 were forcefully sterilized (removal of sex organs) and sterilization was ‘legalized’ in almost 27 states across America. The worst came when the highest court in the US, the Supreme court, passed with a unanimous majority of 8:1 to legalize sterilization. The judge infamously said, “three generations of imbeciles are enough” Unbeknownst to many, the roots of the Nazi’s eugenics movement originated from the US. Nazi’s, however, took it a notch further; from sterilization to extermination.
Science was used as a pawn to further a political or cultural agenda. The eugenics movement is not just a blemish on American history, but human species as a whole.
2. The Opioid epidemic in US
The chapter traces the history of opioid use, and how we ended in this terrible state of affairs. In America, over 130 people die a day from opioid-related and opioid overdose. In 2018, around 48,000 people died from opioids.
Opioids are safe when used in short term for pain relief, but they are highly addictive and end up being misused. Morphine and heroin are extracted from the opium poppy plant. And later on came the powerful synthetic or man-made derivates (Oxycodeine, Fentadone, or methadone - 1000 times more powerful than morphine). USA prescribes 80% of the world’s opiates.
Russel Portenoy’s, one of the leading pain experts in the 70s, seminal paper with just 38 cases claimed that opioids are not addictive and could be used in non-cancer chronic pain patients. Within no time, pharmaceutical companies (mainly Purdue Pharma) aggressively marketed opioids as safe and ‘non-addictive’, and doctors started prescribing these in large numbers. Worse, they even had it going that addiction was not because of the drug, but your ‘personal’ failing.
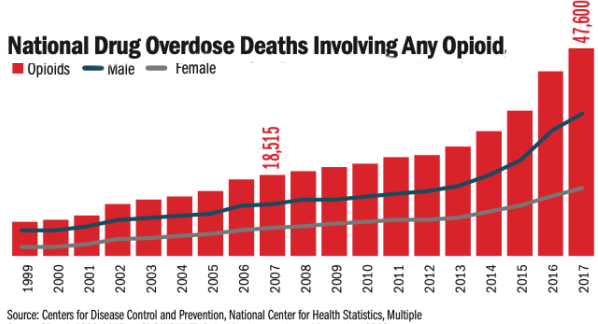
The bottom line is that the data for the safety of opiates was very weak. But data don’t make decisions. I personally think it shows failure at every level: Pharma companies share a major blame for their lies, but also the FDA for approving it for long-term use without vetting the data. And maybe a small part by physicians for blindly prescribing these.
Clearly, one of the worst medical mistakes of modern medicine.
3. The fall of the greatest chemical
Malaria: One of the deadliest diseases in human history. Each year more than 500 million people are affected and more than a million die every year, mostly children. 60% of malaria cases occurring among the poorest 20% of the world’s population.
Now comes DDT- the star chemical that is highly effective against malaria. Besides the effectiveness against malaria, DDT also reduced other fevers like Dengue and yellow fever. It is often said that DDT probably saved more people (in millions) than any other chemical ever known to man.
Then came the groundbreaking, best-seller book “Silent Spring” of 1962 by Rachel Carson, a marine biologist turned nature writer, who helped start the modern environmentalist movement. Unfortunately, her book was loaded on anecdotes and less on science. For example, she based on a retired bank watcher’s anecdote to show eagles were dying because of DDT! Largely inspired by the book and the public uproar that followed, DDT was banned in 1972, and more than 30 nations followed. And malaria came roaring back.

In 2006, the WHO, realizing its mistake, reversed its decision on DDT. Studies show that DDT didn’t cause liver disease, premature deaths, or leukemia as claimed. Extensive research has since shown that well-managed indoor residual spraying programs using DDT pose little harm to wildlife or to humans.
Carson’s basic premise that man-made activities are destroying the environment is correct and should be applauded. Unfortunately, she was wrong about DDT. And a few would argue that her claims against DDT might have lead to the death of thousands, maybe millions.
Conclusion
I love these stories; these stories, as tragic as they are, are a powerful reminder of why we should rely on evidence when claims are casually thrown around, and why we should rigorously evaluate the evidence behind these claims.
Thank you for reading.
Related Articles
4 Things I didn’t Know About Scientific Studies
June 28 2020
Here are 4 important points that I learned about scientific studies that may help you to interpret a study. There are more, but these are the ones that most people miss or ignore, including researchers.
1. Did they use surrogate outcomes?
Years back I thought that any outcome related to the condition or the question is appropriate as long as it comes from a scientific study. Little did I know that there is a hierarchy of outcomes.
What are surrogate outcomes? These are outcomes/endpoints in scientific studies that are just laboratory/physiological markers or substitutes for clinically meaningful outcomes (or outcomes that people actually care about). If you are confused, these examples might help:
What is the harm? We have 100’s of studies that show how surrogate outcomes can be very misleading. In other words, treatment might show positive results in surrogates, but you might see no change in meaningful outcomes or even increased harms. For example, drugs lowered irregular heartbeat, a surrogate outcome, after a heart attack, which is great; we all thought. But tripled deaths. Antioxidants decrease oxidative stress and inflammation which is great but also reduced muscle mass. Testosterone has shown to increase muscle mass in the elderly, but shows little changes in function.
So why are they still used? The majority of the studies use them because these can be gathered rather quickly and cost much less than looking at long-term outcomes such as a disease or death that could take years requiring large samples. They serve well as preliminary data or to generate hypotheses or proof-of-concept trials. But that’s about it; they cannot be used to make a recommendation. That been said, some surrogates are strongly correlated and in the causal pathway, but very few (blood pressure, but still not 100% reliable).
I don’t know who said this, but most patients only care about two simple questions: will I live longer or feel better?
2. What type of evidence/study is it?
If you think every scientific study is equally true, then this one is for you. I used to think this way too. And I will name this the “scientific study bias”.
Simply put, there are different types of study designs and how much trust or credibility we can place on the study depends on the type of study design. As we go down the pyramid, the less we can trust the evidence.

Just to give an example of how little we know about human body: It takes years of in-vitro and animal research or basic science studies by some of the best scientists to come up with a new drug. And once they finally get there, the drug will be permitted to be tested in humans in 4 phases that could take a decade or so. And guess how many drugs make to Phase 1? Just 10%. Or 90% of the drugs fail before even getting to just Phase 1. How is that for the failure rate? For cancer drugs, this is around 3-4%. And this gets worse. Out of the 10%, just 10-20% make it to Phase 3. And even after the drug gets approved and is in the market, they still can be rejected or pulled in Phase 4. And with all this testing, the majority of these drugs are just slightly more effective than a placebo. Also, this “success rate” is considering all the shady things drug companies are notorious for. And in breaking news. we just successfully shot a rocket to space last month, but we still haven’t found a cure to Covid which is killing thousands all over the world (rocket science is hard; medical science is just harder). The bottom line is that the evidence from these studies is not very trustworthy for making health/medical decisions. We may get there one day where we can solely rely on physiology/mechanisms, but we are not there yet for sure. So beware of claims based on these type of evidences.
3. Were the results clinically significant?
I was very familiar with statistical significance or the p-value (are the results due to chance?) since you always see those in an abstract, and it is always taught in our stats classes.
What is it? However, clinical significance is less talked about, and you will never see it in an abstract. It asks, “is the improvement ‘big enough’ to make a meaningful impact in people’s lives (which is why we do research in the first place, right)?”
Any examples? For example, my study shows a 10% statistically significant (P less 0.05) increase in strength or the time taken to rise from a chair in older adults after 12 weeks of exercise training. And the study is statistically significant; hence positive and everyone is happy. But what difference does it make in the lives of my participants? Or in other words, how much of an increase in strength is enough to show an improvement in the quality of life or their everyday functioning? In the multi-million dollar LIFE study, it was considered clinically significant if participants could walk 400 m in 15 min by walking between 2 cones in a long hallway- measure of walking disability. Indeed, more people in the exercise group could do it at the end of three years compared to the non-exercise group. But does it really tell us they had a meaningful improvement? Can they now take the bus or walk a quarter-mile outside and go meet their long-time friend? Maybe. Maybe not. For weight loss, a clinically significant weight loss is around 5-7% of your body weight. But majority of the weight loss studies are often statistically significant, but not clinically significant. So always look at the clinical importance of the outcomes of a study, even if the outcomes are meaningful.
4. Did they control for researcher biases?
Researchers are humans and almost all, including myself, are “biased” towards a favorable, positive or interesting findings. Most people are familiar with the financial conflict of interest (COI), but there is an intellectual conflict of interest that is very hard to disentangle. This was something I never really understood until I started research and publishing (I am not talking about misconduct or fraud or falsifying data, which is cheating and is quite rare).
Why this bias? Study results that are positive or interesting or exciting get quickly published, in better journals, get more “likes” and ‘praises’, gets shared more, and lead to new papers and overall makes the research team very happy. Also indirectly lead to other important incentives like tenure, promotions, and preliminary results for the next big grant. Most of the big researchers in most major universities in US are funded by grants. No grants, find another job. Also, our reward system in research incentivizes publication numbers or quantity and exciting results, but not the methodology or the quality of the paper. Quality suffers when quantity is the focus. The constant mantra in research is “productivity”; quality is the forgotten child. For instance, just look at the number of studies on HCQ against Corona, but the majority of them are just low quality and useless and only serve to create more confusion.
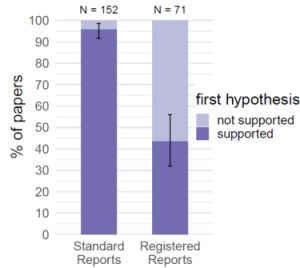
In fact, quality or risk of bias measures like blinding of assessors, concealed allocation (selection bias), pre-registration (reduce selective reporting and p-hacking), blinding data analysis, funnel plot analysis (publication bias), data transparency are all measures to prevent or minimize researcher bias. High-impact journal in medicine are more often than not higher quality and covers most of these biases. Then again, these are million dollar studies, so it is expected. And all that I wrote above is known for years and is not just from my personal opinion/experience. The graph from a recent study shows how registered reports affects the number of “positive” studies.
There are a few more points I wanted to write, but I will end here to give ‘quality’ the last word.
Conclusion:
So next time you read a study, ask yourself:

Related Articles

Is Interval Training the Magic Bullet for Fat Loss?
August 08 2019
This was a recent study that made some headlines looking at at the optimal mode of cardiovascular exercise to lose fat. If you think you need to lose some fat, check this out.
What was the study about?
They compared two modes of cardio: Interval training vs continuous training using a study design called a meta-analysis.

Meta-analysis: Instead of a single study, a met-analysis is simply a collection of previously conducted studies to make one large study. Generally, the conclusion drawn from a ‘well-done’ meta-analysis is more believable or credible than a single study. The simple logic is that the chances of one study being wrong are high, but that of multiple studies being wrong are low.
Interval training: The meta-analysis looked at studies which compared interval training to regular continuous training. So what is interval training? Interval training involves bursts of high-intensity work alternated with active rest intervals. For example, running for few minutes paired with walking. A few types of interval training are:
Continuous Training: This is the traditional form of cardio that most people are used to in which we run or cycle continuously at a moderate intensity for 45-60 minutes.
What studies did they include?
Briefly, the meta-analysis included only studies in English, were at least 4 weeks in duration. had interval training or sprint interval training compared with moderate intensity continuous training, and had measures of body fat.
What were conclusions?
After the inclusion and exclusion criteria, 36 studies were selected for analysis. The conclusions from the abstract:
My Comments:
Most people who read the abstract jump to the conclusion that interval training is the way to go. However, here are a few points that might make you rethink your conclusion:
28.5% reduction in fat: As they conclude, the interval training group lost 28.5% fat mass than continuous training. Sound impressive, isn’t it? But how much fat loss are we talking about. 28.5% means 0.45 kg of fat! Guess what, it doesn’t sound that impressive now. The lesson here is beware of impressive percentage reductions or increases; it may not mean much.
Interval training & time: Arguably the major benefit of interval training is that it is time efficient. So how much difference did they see in time? The average duration for Interval training was 28 min and that for continuous training was 38 min. So you save just 10 minutes! I saving 10 min worth the discomfort and risk of injuries?
Adverse effects: One of the negative effects of interval training is the fatigue and injuries that comes along. They mentioned it, but did not evaluate it quantitatively. Adverse effects are very important when we are talking about high-intensity training (researchers take note pls). Unfortunately, most exercise studies do not report adverse effects in a systematic manner. It s also important to consider that most people do both strength training and cardio whereas in the studies they only performed cardio. So the fatigue will be lot higher than if you are performing interval training and weight training.
8-12 weeks studies: What is abundantly clear after decades of weight loss research is that losing weight is easy, keeping it off is THE real challenge. It reminds of the that famous quote by Lincoln, “It’s Easy to Quit Smoking. I’ve Done It a Thousand Times”. If people are aware of this fact, there would be less number of diets and less number of folks arguing about the best diet. And all these 6-12 week studies are just examples of weight “loss” and says zilch about weight maintenance, which is the real problem. And weight maintenance requires lot more than just exercise!
Exercise & weight loss: One of the major reasons exercise is recommended for weight loss is to reduce the loss of muscle that happens with weight loss. Calorie restriction, and not exercise, is the primary strategy for weight loss. Unfortunately, this study did not look at muscle mass. Considering the higher intensity, interval training may have maintained greater muscle mass which is important (maybe more important than fat loss).
Study quality: What was the quality of the studies? The quality of the studies was low. They did not mention it in the abstract, but when the study quality is low, take the results with a grain of salt.
Exercise benefits: Finally, now there is more and more research showing that exercise has number of beneficial effects that is independent of weight loss. So even if you are not losing weight, you are still reaping a number of neurological, psychological, metabolic and cardiovascular benefits that no pill can claim. Please do think about those when you exercise.
Could you give some tips and examples for interval training?
Of course. Based on research studies:
Commonly used interval training protocols:
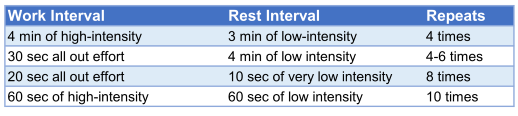
So what should I do to lose weight & keep it off?
I would say the three things that you should focus if losing fat and keeping it off is your goal:
Conclusions
Related Articles




Should You Eat Eggs or Not?
May 16 2019
This recent, controversial study was published in JAMA and was all over the news and social media for weeks. Some folks outright dismissed the study, some were more confused, while a few took a moderate stance. So which approach is right? Here I am going to use an evidence-based approach to answer this very question. So here we go:
What was the study about?
Association: The study was looking at the relation or association of eggs on cardiovascular disease and death in US adults. For this the study combined data from 6 studies from 1985 to 2016 that resulted in almost 30,0000 participants who were followed for a median duration of 17 years.
So why just association and not causal? The reason is that in an observational study, the researcher just “observes” people, for example, in this case, people who eat eggs and those who don’t, and after many years see how many people end up with heart disease or die. As expected, the problem with this type of a study design is that the people who consume eggs might also have other unhealthy habits such as eating red meat, smoking, eating junk food, being sedentary and so forth. That means, people who eat eggs and those who don’t might be different in a number of ways. Consequently, we don’t really know what exactly caused the heart disease; is it the egg or some other unhealthy habit(s) they have. To overcome this problem, researchers commonly adjust for these differences using statistical techniques, but nobody is sure how well we have adjusted for these differences. Hence the reason why it is said that observation studies can only show association and not cause and effect.
Adverse effects/harms: On a passing note, observational studies cannot show cause and effect, but it’s important to note that adverse effects or harms can only be really studied using an observational type of study design (ethical, financial, & logistical reasons), So observational studies assessing harms shouldn’t be just casually dismissed unless you have a better way to study harms/adverse effects. Do you?
So what were the results of the study?
What about the quality of the evidence?
Or, in other words, how certain are we about this relationship. One of the critical aspects in evidence-based approach is to grade the quality of evidence. There are number of grading schemes out there; one commonly used approach is to grade the evidence into: Very Low, Low, Medium, & High. And the higher the grade assigned, the greater the trust we can place on the evidence.
Observational: Of course, being observational is one of the major limitations of the study. So that means, we don’t really know for sure if the increase in heart disease is really due to eggs. In an evidence-based method, observational studies are graded always as low-quality evidence.
That beeing said, the study do have some major strengths:
Dose-response: One of the major strengths of this study is the dose-response effect. The results showed that the more eggs you eat, the higher the risk of heart disease and death. So if you had 2 eggs per day, your risk went up by 27% for heart disease and 34% for mortality. Mind you, a large reason why cigarette smoking and lung cancer is considered to be causal is because of the large effect on cancer and also the dose-response effect observed. Here, we have a dose-response effect, but the magnitude of effect on heart disease and mortality is very low.
Individual participant data: Also, this study used individual participant data (IPD) rather than average of each studies. So it is akin to one large study of six studies with data available from each person. In turn, this makes the study and statistical adjustments that we previously mentioned highly reliable than previous studies on this topic. Almost all articles have missed this important point. Thus, this study is the “best available evidence” we have on this topic.
Quality: Taking into account the dose-response effect and the observational nature, we can say that the study is of low to moderate quality. Or we only have a low to moderate confidence in the evidence, at best.
What about the benefits of eating eggs?
Benefits: Eggs as many are aware are nutritious, high-quality source of protein and B vitamins, and relatively inexpensive. That been said, there is little evidence to show that eggs have any critical benefits in terms of longevity or disease prevention. On the other hand, the risk is a small increase in heart disease and mortality that we are not so confident of.
So what recommendation can we make?: The bottom line is that we can only offer a weak recommendation against eating eggs. Or any recommendations made against eating eggs are just ‘suggestions’ and ‘contingent’ on the individual circumstances and preferences. On the other hand, strong recommendations are given out when we have very high confidence in a large risk vs benefit ratio.

So what is the controversy regarding cholesterol?
Cholesterol Cut-off: The 2010-2015 Dietary Guidelines of US recommended a cut-off of 300 mg. However, in the 2015-2020 updated guidelines, they removed this cut-off and instead stated “as minimum as possible”. So although they took off the quantitative limit, cholesterol is still a nutrient of concern.
What made everyone a bit confused was that they wrote “No appreciable relationship between dietary cholesterol and serum cholesterol or clinical cardiovascular events in general populations” and at the same time paradoxically wrote “Individuals should eat as little dietary cholesterol as possible”. I do think this will be changed in the upcoming guidelines. Just keep in mind that one egg yolk has around 186 mg of cholesterol.
So should I stop eating eggs or what?
Taking into account, the small risk, low to moderate quality of evidence, we can only offer weak recommendations or suggestions against eating eggs. Some of my ‘suggestions’ for people who eat eggs:
Clearly, the recommendations vary depending on the individual circumstances and preferences. Finally, as you can see, evidence-based approach is more than just reading the study results and jumping to recommendations. In contrast, EBA involves finding the best-available evidence, grading the quality of the evidence, understanding and communicating the risk/benefits clearly, and then conveying the strength of your recommendation. Thank you for reading.
Related Articles

Do Training Masks Improve Performance?
February 02 2019
You might have seen folks training in the gym or outside wearing these masks. Admittedly, they do look cool and high-tech, but do they have any benefits?
What are the benefits of training masks?

The makers claim better fitness and improved performance in a wide range of activities
Performance: Quoting from their website:
“Training Mask is used to improve your breathing power and technique so that you can perform better in a broad range of physical activities such as running, weight lifting, sports, yoga, and core exercises. Performance breathing with Training Mask has multiple benefits that lead to improved athletic performance and better fitness (www.Trainingmask.com).”
Image Credit: Trainingmask.com
How do training masks work?
According to the website:
“Training Mask reproduces hypoxia at a fraction of the cost of multi-thousand-dollar altitude training chambers, or expensive trips to the Rocky Mountains. “The Training Mask Effect” is a proprietary combination of Resisted Breathing & Hypoxic Training”
Basically, the mask ‘works’ by mimicking high-altitude training and by training your breathing muscles.
Are there any scientific studies?
In their website, they have referenced 2 studies that both gives the impression that these mask do work. But do they?
Aerobic Exercise Study 1: In study 1, twenty-four moderately trained subjects were divided into a training mask group and a control group and trained on a cycle ergometer for 6 weeks. Two variables (unlike the 4 shown on the site) showed significant difference (out of 14 variables measured).
- Major Limitations: First, the study measured everything except the most important variable - performance. People care about the mask because it is claimed to improve performance, not because it improves a couple of physiological variables. Second, the control group did not wear a sham mask during training. Considering the vo2 max test involves breathing through a mask as the final test, a group that trained using a mask will have an unfair advantage. So improvement even in some of the markers is questionable.
Weight Training Study 2: In study 2, they showed that weight training increased growth hormone and muscle thickness in the hypoxia group (low oxygen group).
- Major Limitations: Unfortunately, the major problem of this study is that they didn’t use the training mask. The study participants inspired hypoxic gas (14.5% oxygen corresponding to 4000m sea level) to mimic low oxygen levels. That is, you will need a mask and an oxygen tank! So the website is partially correct.
Bottom line - none of the studies cited support an improvement in athletic performance as claimed.
Is it similar to altitude training as they claim?
Altitude training mechanism: At high altitudes, the thinning of air leads to a lack of oxygen (called hypoxia)that triggers the release the hormone Erythropoietin. This hormone increases our red blood cells (RBC). And since 95% of the oxygen in our body is carried by RBC’s, the increase in RBC means greater oxygen carrying capacity and better performance.
Mask vs Altitude training: The mask simulates altitude training by reducing the air you can breathe. So the company is right to claim the mask leads to a hypoxic environment. However, the problem here is the degree of hypoxia needed to achieve an increase in RBC’s. In the first study, the oxygen levels in the mask group decreased by 2%. On the other hand, in altitude training, the reduction in oxygen levels is as high as 40%. Hence the reason the aerobic study didn’t observe an increase in RBC’s with the mask training. And importantly, the increase in RBC seen in altitude training requires hypoxia for 12-22 hour/day, which requires athletes to live at high altitudes for weeks. In short, unless you are Batman and wearing the mask the whole day, I just don’t see the mask improving your red blood cell count.
Live High, Train Low: Due to the low oxygen levels at high altitude, training intensity suffers. To overcome this problem, athletes live at a higher altitude to improve their blood RBC’s and train at lower altitude to maintain their intensity. This lowering of workout intensity is a problem with mask training. In fact, one weight training study has shown to decrease performance or the repetitions performed during squat (3-4 repetitions). Another one showed significant decrease in alertness and focus for task in the mask group.
So how can I improve my breathing muscles?

Respiratory muscle training (RMT): RMT involves training your respiratory (inspiratory or/and expiratory) muscles by breathing into a pressure device for 15-30 minutes, 3-4 times per week. Apparently, unlike the mask, a number of meta-analysis (group of studies) have shown RMT to enhance performance (Timed trials, Endurance time) in non-athletes and athletes from multiple sports (rowing, running, swimming, cycling, Intermittent sprint sports). And since you re not using this during training, it doesn’t negatively affect your training either.
Conclusions
Reference 1, Reference 2, Reference 3, Reference 4, Reference 5
Related Articles





Is high frequency better than low frequency to improve muscle and strength in trained lifters?
December 14 2018
Here is a recent study that compared 6 days/week to a 3 days/week workout program on muscle mass and strength in trained lifters.
Why did they do the study?
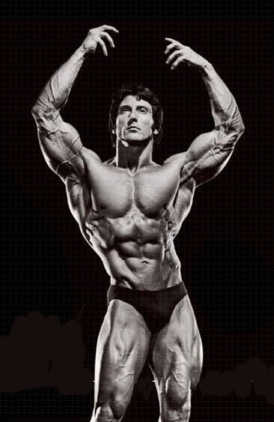
Photo Credit: Muscle & Strength, LLC
So the question is whether high frequency is better than low frequency in trained subjects in improving strength, muscle mass for a duration of 6 weeks.
What were the methods?
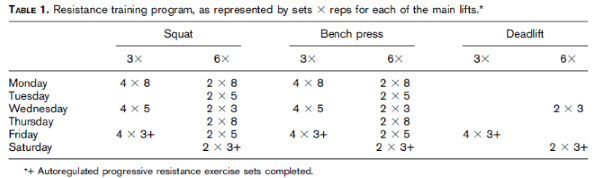
What were the results?
What was the conclusion?
High-frequency (6/week) resistance training does not seem to offer additional strength and hypertrophy benefits over lower frequency (3/week) when volume and intensity are equated.
My Comments
Here are some of the aspects of the study that I thought was worth mentioning:
Hypothesis: The hypothesis of the study according to the authors is ” .. an increased training frequency would not lead to further improvements in strength and body composition when compared with a lower training frequency…”. That means, there will be no difference between the groups.
Drop-Outs: In the high frequency group, out of 23 assigned, 11 dropped out.That’s a 50% drop-out rate in 6 weeks! And it is very surprising that the authors thought this was not important to discuss in the paper, let alone report it. If I had to peer review, that would be my first question in a high frequency study.
In short, a study should analyze all the participants that were randomized in the beginning. If there are drop-outs, they should tell us why they dropped out. Here the participants dropped out either because the they couldn’t workout 6 days/ week or had adverse effects or their results were not as expected. If the latter, then the high frequency could be worse than a traditional 3 day/week program. So considering the large drop-out from the high frequency group, there is a high risk of bias in this study.
Muscle Mass: One of the rationales for high frequency workouts for muscle growth is that protein synthesis comes down quickly in trained compared to untrained. In theory, at least, that suggests a higher frequency could be better in trained lifters. Fat-free mass showed 0.9 kg (2.5, 0.7) difference in favor of the high frequency group: A 2lb improvement in fat-free mass in 6 weeks is indeed a large improvement. But mind you, this improvement could be as high as 1.7lbs in the 3 days/wk group too if we repeat this study! Also, they used an A-Ultrasound for measuring muscle mass which is a cheaper version of the B-mode ultrasound and has questionable validity.
High-level weight lifters: In the introduction, the authors mention elite level weightlifters splitting their workout to support a high frequency workout. And it is true many weight lifters train a lift 6-8 times per week. Unfortunately, elite level lifters are a classic example of selection bias. What you see are those 1% of athletes who survived the brutal training and competition in their lifetime, especially the ones on a high frequency training program. That means, the rest of them either got injured/plateaued/quit the sport. And this is exactly why you shouldn’t copy elite level athlete’s program or use them as a rationale for a scientific study on average lifters.
Also, elite lifters have their nutrition, recovery, coaching, and rest almost close to perfect. Most of these lifters are professionals that means they only train and sleep. And unlike the participants here, these lifters might have taken years to slowly raise their frequency to their current level. This is just staggeringly different from college going students who participate in studies because they can earn a few dollars or a class credit. So be wary of elite level lifting programs.
Adverse effects: Any adverse effects like injuries or fatigue from training 6 days/wk? We have no clue since the authors did not bother to report them. What about attendance in each group?. Did they show up for the 6 day/wk workouts to actually claim high frequency? Again none reported. Any limitations reported? I thought they would certainly have a few limitations to talk about. I was wrong. None mentioned.
What if you want to try high frequency workouts?
Here are some practical tips so that you don’t kill yourself:
As a final note, critical thinking shouldn’t stop when you stumble upon a scientific study (as many do). In fact, critical analysis only begins and happens to be one of the fundamental steps to interpreting a study. And this is true even for my ‘impeccable’ studies.
Conclusion
Related Articles




American College of Sports Medicine 2018 Conference Review Part 1
June 23 2018
The 2018 annual American College of Sports Medicine (ACSM) conference was held at Minneapolis from March 28-June 2. For people who are not aware, ACSM conference is the largest conference in the exercise and sports medicine area. I stayed at the Normandy Inn, which is a 15-minute walk from the Minneapolis convention center.

The conference officially started on Wednesday although there were pre-conference talks on Tuesday. They had 5 different tracks to choose and each track had number of talks going on at the same time.
Physical Activity for Cancer Prevention and Treatment: State of Evidence
The first highlight talk in the morning essentially summarized the evidence from the, yet to be officially released, federal physical activity guidelines for cancer prevention by Dr. Anne McTiernan at Fred Hutchinson Cancer Research Center, Seattle. The last physical activity guidelines came out in 2008, so this is a major update that everyone was eagerly waiting for. The new guidelines will be officially released by the end of 2018.
Some of the main highlights of the talk:
What about areas for future research:
In short, please exercise if you want to reduce cancer risk. We all know the “Relay for life” runs to raise awareness and money for cancer research. But I seriously don’t think a lot of people think they are doing a lot more in preventing cancers for themselves by just participating in these charity runs. And this is why it kills me when people talk about exercise just merely in terms of losing weight and looking good. So remember this next time you exercise.
Hypertrophy: The Extrinsic Variables
This symposium was on the topic of muscle growth. I could never find the rooms where the talks were held and always got lost in that big convention center.
The first talk was by Dr. Michael Roberts from Auburn University. The talk was about how muscle mass is measured and how it is defined. DEXA which is commonly used to measure muscle mass counts extracellular water as muscle too. He showed a slide where subtracting extracellular water measured using Bioimpedance spectroscopy drastically reduced muscle mass measured using DEXA. And he was just talking about,extracellular water, but remember that muscle is 70% water. He concluded by saying estimating changes in extracellular water is important when assessing muscle hypertophy and we need to address “what hypertrophy is”. In fact, my recent grant was on this same topic but in older adults. It may sound academic, but it has a lot of implications on defining clinical cut-points for sarcopenia.
The next talk is from our very own Dr. Brad Schoenfeld - a.k.a Dr. Muscle from Lehman College. Brad talked about the myth of an optimum repetition range for muscle hypertrophy. He started off by talking about studies on protein synthesis showing that high reps and low reps producing similar results. He then talked about results in untrained individuals which didn’t really convince him and how it prompted to do his own study on trained (I have written about this study in another article). And finally he did a meta-analysis (collection of studies) showing high reps and low reps to be both effective in increasing muscle. Interestingly, he also said there is some evidence to show higher reps might be targeting more of the Type 1 and lower reps the type 2 fibers. I thought Brad had a nice progression in his talk - from basic science to single studies to finish off with a meta-analysis. Can’t argue with that logic, can you?
The next speakers were Jeremy Loeneke and Jeremy Steele. But I had to leave since my poster session time was up. My poster was on the energy cost of walking in older adults. We know the energy cost for walking in old people is low. But we wanted to see this in low functioning old people. This was part of a big NIH study that I am involved in. Briefly, low functioning older adults walk slowly compared to healthy older adults, but they tend to burn similar calories. And this partly due to their lower cardiorespiratory fitness (vo2peak). So they are walking very slow, but still struggling and burning more to do that even. It could also be due to compensations, neurological, muscular and so forth too.
Supplements to Promote Hypertrophy and Combat Atrophy
Creatine
I was a bit late for this talk since I was at the poster presentation. I walked in to the presentation on creatine by Dr. Eric Rawson from Bloomsburg University. If I heard him right, he said most of the effects of creatine were due to people working harder than the direct effects of creatine per se. He also mentioned that creatine do not exacerbate muscle damage, even with intense damaging protocols, and helps reduce inflammation and improve recovery. Creatine monohydrate is nearly absorbed 100% so increased absorption with other creatine formulations are just outright scams. Creatine upregulates or expresses a number of growth related genes, GLUT-4 and improves carbohydrate metabolism and such. One of the audience comments was the role of creatine in increasing water content through improved glycogen stores is under appreciated. Mind you, one gram of gylcogen stores around 3-4 gms of water along with it.
Fish Oil
Dr. Bettina Mittendorfer from Washington University in St. Louis talked about the effect of fish oils on muscle hypertrophy. She talked about how fish oils have showed increase in protein synthesis in both old and young adults. And how fish oil supplementation have shown to increase muscle mass and physical performance in older adults. I thought she could have mentioned some of the negative studies too because there exist a few. For the Q&A session, I asked what is driving this increase in protein synthesis. She replied that she is not really sure and the increase in protein synthesis was independent of the anti-inflammatory effects of fish oils. Fish oil is getting a lot of flack these days due to the null effects on cardiovascular outcomes. But the effects of fish oil on the muscular system are very novel and interesting. And on a related note, I just submitted a fish oil paper to one of the major medical journals.
Now for some closing thoughts: The more I learn about research and the more I attend these conferences, especially being in the midst of a replication crisis, I think presenters should spare some time to talk a bit about study quality and limitations. I always tend to enjoy poster sessions at conferences; it is just one of those rare occasions where you can learn about the study and have the study author to answer your questions right in front of you. It was also so nice to see all these students from so many far away countries talking about their little study with so much passion and confidence. That always puts a smile on my face.
That’s all for the first part. In the second part, I will review some of the other interesting talks and posters that I came across. Thank you for reading.
Related Articles

International Frailty and Sarcopenia Conference 2018 Review
April 01 2018
Here is my review of the sarcopenia conference held in Miami Beach on March 1-3, 2018.

As the name suggests, the conference is aimed at understanding age-related muscle loss and frailty. This my first time attending this conference, and compared to other conferences, the scope is quite narrow and only attracts a small crowd of 500-700 attendees. The conference seems to go all over the globe and has a lot of international attendees. Last year it was held in Barcelona, Spain. So off goes me and my mentor to the sunny Miami Beach.
This was a 3-day conference so there were quite a few presentations. Below are the some of the presentations I attended and thought were noteworthy to write about.
Frailty
The key note speaker was Linda Dr. Linda Fried, the Dean of Columbia’s University’s (NY) Public health department. In fact, she was also honored with Lifetime achievement award at the conference. And her work was instrumental in defining frailty and bringing frailty to the forefront of clinical research. Her keynote lecture was on what has been done on frailty and what needs to be done
Frailty is condition that is barely known to many; at least I wasn’t until I stated my post doctorate. Frailty is defined as a distinct condition/phenotype that is indicated by the presence of 3 out of 5 conditions: muscle weakness, slow gait, low physical activity, low energy or exhaustion, and unintentional weight loss. It is not a disease or a group of disease or disability as some of us might think. If you can think about anyone who is old, thin, slow, weak, and sedentary, then you have come across frailty. Almost 7% of people in US are frail and we don’t really know what causes frailty. Below is the cycle of frailty from her paper.
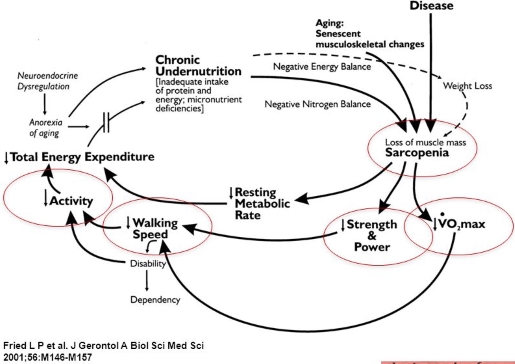
And which is the best way to prevent frailty? I will give you one guess.
Muscle Stem Cells & Aging
Next talk was by Charlotte A. Peterson at University of Kentucky, Lexington about role of satellite cells in sarcopenia. Her research showed that the lack of satellite cells or their activity was not a contributing factor in sarcopenia. One of the prevailing hypothesis is that the lack of satellite cells/stem cells could contribute in older adults.
However, I have to say her experiments were in a mice model and goes counter to some of the recent human pilot showing favorable effects on function with stem cells infusion. In fact, a phase 2 study funded by NIH is currently looking at the efficacy and safety of stem cell infusion in humans to improve function. Just like many people would say, conclusions from animal studies should stay within the realm of animal studies and only serve as a hypothesis for human studies.
ENRGIZE Pilot Trial
Next in line was the enrgize trail: Dr. Marc Pahor (Director of Aging, Institute at University of Florida) talked about the design and rational of the study while Dr. Manini (my mentor) introduced some of the baseline association in the study.
The Enrgize is a 10 million, multi-center, double-blind, 1-year pilot trial which randomized 300 older adults with high inflammation and low walk speed into 3 groups: fish oil, losaratan and a placebo group. (and yes you read it right “10 million-dollar pilot trial”).
The rationale for the study is that the decline in physical function in older adults has shown to be related to age-related inflammation ( IL6, TNf-alpha, CRP). So if we can lower this low-grade inflammation, we may prevent the decline in function in older adults. We are the coordinating center and it is just amazing to watch the rigor involved in this study, especially due to the multi-centered nature of the study.
The baseline results showed statistically significant association between leg extension strength and fish oil supplementation, but not for other measures of function. The study is in the final stages so we will know something soon.
SPRINTT Trial
The SRINTT trial is a large clinical trial spanning across 11 European countries looking to see if a multi-modal intervention (physical activity, nutrition) can prevent walking disability in older adults who are both pre-frail and sarcopenic.
Although there are few differences, the trial is very similar to the LIFE trial conducted in US and will serve as a replication of the LIFE study. The main difference between the LIFE are that in the SPRINTT are that in the SPRINTT the participants have low muscle mass measured using DXA and the intervention will include a nutritional component. I review the LIFE trial here:
The study finished recruiting and randomizing 1500 participants and the intervention is currently underway. The presentation showed some of the baseline characteristics of the participants and screening rates at different centers.
Capillarization & Muscle Growth
The was one interesting talk to say the least. Capillarization means the increase in blood vessels in the muscle. The increase in capillarization is usually considered to be an endurance training adaptation, and aging somehow tend to decrease capillarization.
In one of their resistance training studies in older adults, type 2 muscle fiber hypertrophy was observed only in the subgroup who had high capilliration, whereas no increase was observed in the low capillarization group. Further, they also showed greater satellite cell activity and proliferations in muscle fibers with higher capillarization.
Does the relationship hold true in younger folks? So endurance training good for increasing muscle?
D3-Cr
Deuterated Creatine (D3Cr) is a novel, emerging method to measure total body muscle mass. The method involved estimating muscle mass from creatine levels from fasted urine, after consuming a deuterated creatine capsule. Notably, unlike DXA to measure muscle, D3r can distinguish actual muscle tissue from hydration levels, connective tissue and intramuscular fat.
Dr. Peggy Cawthon showed some preliminary results showing the superiority of the method compared to DEXA for some measures. In fact, the pilot grant (100K) I received recently is based on this novel method. If the method turns out be as promising as the preliminary results, it will definitely change the way we measure muscle mass in the future.
Dynapenia & Serious Fall Injuries

My poster (shown here) was on the association between dynapenia (loss of strength) and serious fall injuries. We know strength loss to be a major risk factor for falls, but the role of strength on fall injuries is less clear. We also used the new grip strength guidelines developed by FNIH to diagnose weakness. Although it is been known for years that strength loss is a risk factor for falls, we are still struggling to settle on a cut-off point to diagnose muscle weakness and make treatment recommendations. And from what I understand talking to my mentor, the new classification doesn’t look that promising either.
Overall, the conference was very well organized and gave a glimpse of where the research on sarcopenia and frailty is currently at and heading towards. I wish they could have had a dedicated time for poster sessions. Unlike other conferences I have attended, there was no allotted time for posters so there was no one around the poster to interact/ ask questions. I always looking forward to the posters session for this reason, so was little disappointed to see all the orphaned posters. Another thing I noticed was that quite a few drug company representatives and companies were present at the conference. And I couldn’t help get the feeling that we will soon see a few drugs for treating sarcopenia in the next few years.
Anyway, that’s all I have for the sarcopenia conference. The conference is very expensive ($800 for non-students; $500 for students) so I am not sure I will be able to make it next year. But if you work/interested in the area of aging and physical function, this is the conference to attend and meet some big names.
Related Articles

Can you Cure Diabetes?
December 21 2017
A short post on an amazing study showing some incredible results recently published in The Lancet - one of the leading medical journals.
Why worry about Diabetes?

Diabetes: Diabetes is a disease that happens due to high sugar levels in your blood. In Type 2 diabetes, your body cannot absorb sugar from the blood because it cannot make insulin or use insulin well.
Some ‘interesting’ facts about diabetes:
Why did they do the study?
What did they do?
What were the results?
Diabetes was reversed in 46% (68 participants) of the treatment group and 4% of the control group (odds ratio 19·7). In other words, they came of their diabetic medication because they had diabetes no more! These results are very impressive, to say the least.
My comments?
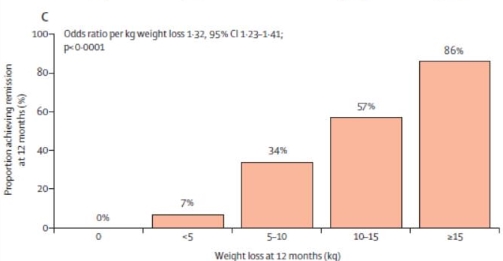
Conclusions
As always Exercise Biology will bring you the latest and most cutting-edge scientific news in exercise, nutrition and health.
Related Articles



What is Sarcopenia (or muscle loss) and how to diagnose sarcopenia?
November 27 2017
Most people have heard about osteoporosis or loss of bone. Surprisingly, very few people have heard about sarcopenia or loss of muscle, which apparently is more prevalent and insidious than bone loss.So what is sarcopenia?
Sarcopenia: As the name suggests, sarcopenia (Sarc means flesh; penia means loss) is the loss of muscle mass as you age. It is now clear that we lose muscle mass at rate of 1-2% per year in both men and women. It is estimated that by the age of 80 you will lose around 40% of your muscle mass!
What are the consequences of sarcopenia?
There are a number of serious consequences of sarcopenia or muscle loss. Some of the major ones are:Now, what leads to sarcopenia?
Some of the factors contributing to this loss of muscle are:Ok great. So how do you diagnose or sarcopenia?
It has been almost 30 years since the term sarcopenia was coined. Unfortunately, we are still struggling to come with a universal definition for identifying sarcopenia. If we can identify folks who are at a high risk of muscle loss, we can treat them better.What is the recommended criteria for sarcopenia based on FNIH

Ok . Now tell me how I can prevent sarcopenia?
What is my opinion on this topic?
Conclusions
Here you go.Related Articles



Cardiorespiratory Fitness: The Key to a Longer Life
July 09 2017
If you ever thought about living longer, then this article is for you.
Why cardiorespiratory fitness (CRF)?
The AHA (American Heart Association) recently released a groundbreaking statement recommending the routine assessment of cardiorespiratory fitness (CRF) by doctors. Finally, we have compelling evidence to show that:
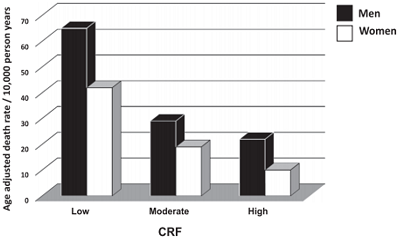
Mind you, America Heart Association (AHA) is the largest non-profit organization dedicated to fighting heart disease and stroke in the US. Most heart-related guidelines and policies you hear about come from AHA. So when AHA release official statements, you better listen
But what the heck is cardiorespiratory fitness?
Cardiorespiratory fitness means the ability or the capacity of your heart, lungs, and muscles to intake oxygen and use it to make energy. The higher your CRF, the more efficient the whole process.
So how do you increase cardiorespiratory fitness?
How to measure cardiorespiratory fitness?

As long you are using a reliable measurement, what matters is the change over time. So you do not need the gold standard to know if you CRF is improving.
Are there any Randomized controlled Trials (RCT)?
RCT’s: If you have been reading this site, you probably know that RCT’s are the gold standard in scientific studies. Currently, there aren’t any RCT’s which show a decrease in mortality and CVD with increased CRF. However, considering the strong associations and the biological mechanisms involved, these results are pretty strong, I think.
Conclusions
The official release of the statement by AHA because of the overwhelming evidence is probably the most important information to hit the exercise and fitness industry in the past decade. In fact, AHA recommends all adults to estimate or measure CRF routinely just like cholesterol and blood pressure. You can be normal weight or “in-shape”, be strong as an oak, eat healthy, or even have a six pack, but you still have a higher risk of mortality or heart disease compared to a person who is normal weight and has a higher CRF than you. People spent thousands of dollars on supplements like Vit C, Vit E, fish oils, organic foods so that they can stay healthy and live longer, but none of these have the benefits or scientific evidence anywhere remotely close to that of exercise. And it literally kills me deep down to know that this hasn’t got enough attention from fitness bloggers and news outlets; this should be the cover story for all fitness organizations and personal trainer’s sites.
As always, Exercise Biology will bring you the most honest and cutting-edge scientific information about health and fitness that you will ever find.
Reference 1
Related Articles
Miscellaneous Thoughts - A Gene to Drug, Rippetoe on running, and March for Science
May 30 2017
Majority of my articles are on one subject so that I can go a bit more in-depth. However, in this article I am writing on 3 topics that has grabbed my interest recently. Hope you enjoy the new format.
The story of a gene to drug
A few weeks back, a blockbuster study was published in the NEJ M (New England Journal of Medicine)- one of the top 3 medical journals. The phase 3 clinical trial- FOURER trial, looked at a new class of drug (PCSK9 inhibitor) to lower cholesterol in patient’s who are on statin treatment.
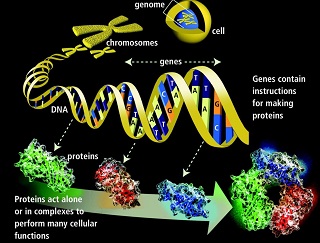
Why statins? Heart disease is the number one cause of deaths globally. Increase in cholesterol levels can increase the chances of heart disease, especially in people with other risk factors. Statins are the most widely used drugs in the world to lower cholesterol. However, in many folks statins can have side effects like muscle pain/weakness or is not effective.
The current study looked at a new class of drugs in people who have both heart disease and are on statins to further lower their cholesterol. Now for some interesting study facts:
But for me, what was fascinating about the trial is the story behind this drug.
The story begins in 2003 when a healthy African-American women walked into a Texas hospital for a leg injury and was found to have an impossible cholesterol level of 14 (the healthy level is below 100) After 1000’s of blood test, they identified that her genome (or gene map) is missing the PK076 gene. In general, people who have a missing gene have severe life threatening conditions. But not her, which made the discovery even more fascinating. Years down the road, and after a number of experiments in cell culture, rodents, phase 1 & 2 human clinical trials, finally in this phase 3 trial the drug works. In fact if you ever wondered about the term translational research, the story of this little drug is an iconic example of what people really mean by translation research - from a single gene to finally having an effective drug in humans. And it is a true testament of the progress in medical science.
Why you should not be running
Now let’s take a quick turn from drugs to exercise: This piece with a controversial title is written by none other than Mark Rippetoe - one of the biggest names in the fitness/strength industry. So it goes without saying his articles usually have a lot of reach and punch.
Although the title sounds like it is just against running, the article argues against any form of cardiovascular/endurance exercise and simply promotes strength training. The author believes that national physical activity guidelines endorsed by doctors and exercise physiologists ignores strength training, falsely emphasizes endurance activities, and correctly-designed strength training’ gets sufficient stimulation of the heart .
And what is his evidence against endurance/cardiovascular training? Endurance training is counter intuitive to muscle adaptations, “excessive amounts” of endurance activities are not good for body. Examples quoted include increased death rate in marathon runners, muscle loss in cyclists, and repetitive motion injuries in runners and cyclists.
My points where I think the article is just completely off.
I dislike cardiovascular exercise, love weight training, and the majority of my published studies are on strength and power, but that will not(or should not) color my recommendations to my readers/clients. Please do both cardiovascular and strength exercises, if health and longevity is a priority.
Ending with a Spiderman movie quote” With great power comes great responsibilities”
March for Science
Running for health to marching for science. On April 22, April 2017, people all over the world marched to defend the role of science in policy and society. In fact, the march is a direct result of the new US presidential attitude towards climate change, vaccine safety and budget for research. It is just sad that we have to organize a march in the 21st century to remind people of the significance of thinking/logic/reason in our lives.

In my opinion, if a politician(s), or for that matter anyone, who has gone through 10 years of school, 4 years of college, and for some, 2 more years of advanced study, has issues interpreting science from junk science, then our education system has to brunt a small chunk of the blame. Seriously, what did we teach them in those 10-15 years? How to memorize and pass tests? Apparently, we taught them everything under the sun, but forgot to teach them the most important lesson in school- “how to think”.
What is ironic (and puzzling) to me is a profession which demands evidence and references for any claims you make as a student, and rightly so, has zero regard for an evidence-based approach when it comes to their own profession. I have yet to come across a professor who uses the latest science of learning or reads studies about how to teach better or how people learn. In fact, I have taught for more than 6 years, but I have never been formally educated or trained about how to teach or how to make your student think critically. The mandatory question in every college teaching job interview ,’what is your teaching philosophy” tells us what is seriously wrong with our education system. If cancer research (evidently more complicated than landing on Moon) depends on an evidence based approach, what’s your excuse?
Anyway, I think I will stop here. I had a few more topics in mind, but it is getting too long. Thank you for reading
Related Articles
Evidence-Based Practice in Exercise & Nutrition: Common Misconceptions and Criticisms
March 03 2017
Introduction: Evidence based practice or EBM is an area that I have always been passionate about.In fact, speaking to the late David Sackett (the father of EBM) about EBM on a few occasions is something that I will always cherish. Without an EBP approach, scientific research in health and fitness is pretty much useless. Even if you are not a doctor or a fitness professional, if you are remotely interested in your health or fitness or nutrition, you should have a basic understanding of EBP. In the article below, I am collaborating with my friend and colleague Brad Schoenfeld, Ph.D. to answer some of the common concerns and questions about EBP. Brad has a strong practical and research background, which is not commonly seen in the fitness field.
We (Anoop Balachandran, Ph.D. & Brad Schoenfeld, Ph.D.) are glad that more and more people are demanding and applying evidence in the exercise and nutrition field. That been said, there remains a lot of misunderstanding and misconceptions about an evidence-based Practice (EBP). In this article, we will address some of the common misconceptions and criticisms of EBP. Here we go:
1. Why do we need EBP? Why can’t we just use anecdotal evidence or expert opinion?
In fact, we’ve used anecdote or expert opinion as ‘evidence’ to treat people throughout the history of medicine. But this approach clearly didn’t work well as shown by hundreds of examples of medical mistakes we made in the past. For example, smoking was ‘good’ for heath until studies showed otherwise; bloodletting was the standard medical treatment for almost 2000 years by the foremost doctors of the West, and so forth. In short, EBP evolved because anecdotal evidence or expert opinion were not producing ‘results’.
You can read more about it here:Why We Need an Evidence-Based Approach in the Fitness Field
2. So what is EBP/EBM?
The definition of EBM (Evidence Based Medicine) by David Sackett reads: “EBM is a systematic approach to clinical problem-solving that allows integration of the best available research evidence with clinical expertise and patient values”. This principle can be applied across many scientific disciplines, including exercise and nutrition, to optimize results.
2. What is evidence?
Many people wrongly assume that the term “best available evidence” in EBM/EBP is limited to research-based evidence. In fact, evidence can be obtained from a well conducted randomized controlled trial, an unsystematic clinical observation, or even expert opinion. For example, the evidence could come from a controlled trial, your favorite fitness guru, or a physiological mechanism. However, the critical point is that the importance or trust we place on the evidence differs based on the type of evidence. We will talk more about this as we talk about the evidence hierarchy.
3. What about values and preferences?
Every patient or client assigns his/her own values, preferences, and expectations on outcomes and decisions.
For example, some might place a high value on muscle growth, whereas others would value their general health as most important. Some would value building their upper body muscles more than their lower body muscles. Others may value the social aspect of working out at a gym more than the muscle and strength gains.
And rightly so, these personal decisions have no wrong or right and should be listened to and respected. The job of a fitness professional is to help clients achieve whatever goals they desire; we cannot impose our own values no matter how contrasting beliefs and opinions maybe.
4. What about clinical expertise? And what is the ‘art’ of EBP that people always talk about?
Clinical expertise is what many refer to as the art of EBP. So, does the art of EBP mean applying what has worked for your clients? Clearly not.
Clinical expertise involves basic scientific knowledge, practical expertise, and intuition to:
And this is called the art of evidence-based approach. As you can see, it forms an integral part of EBP and no amount of research can replace it. Likewise, no amount of clinical expertise can replace research evidence.
5. What is the evidence hierarchy? And why are RCT’s (Randomized Clinical Trial) at the top of the pyramid?
An evidence hierarchy is one of the foundational concepts of EBP. And there are three important points to keep in mind:
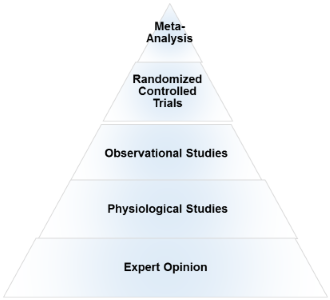
6. What if there are no RCT’s? How do I evaluate a program or diet?
First, as mentioned before, there is always evidence. If there are no RCT’s, you simply move down the evidence hierarchy. But as you go lower in the hierarchy, uncertainty about the validity of the evidence goes up as well. Second, you also must compare the benefits, risks, cost, scientific plausibility, and other alternative programs before making recommendations. Below are a few examples where the absence of an RCT does not preclude recommendations.
What if there are no studies and my client wants to try a new program?
As previously noted, if a person understands the uncertainty due to the lack of studies or weak evidence, availability of alternative programs that fit his/her goal, the cost, and risks, he/she can make an informed personal choice. Keep in mind that majority of the questions in exercise and nutrition are of weak evidence. In fact, it is the same for the medical field too. But what is important is to clearly know and convey what your recommendations are based on.
7. There are a lot of factors like genetics, diet, motivation that can influence your results. A study hence…
Many people are unaware that in a randomized controlled trial, the randomization serves a crucial purpose: The randomization ensures that both the known variables and unknown variables that can affect muscle growth or strength are equally distributed into both groups. That is, if there are unknown genetical factors that can drive muscle growth, it is highly likely these genetically gifted individuals will be distributed evenly. This is the reason why RCT are considered to be the gold standard to study cause and effect. Hence, the results of the study can be pinned to the intervention or treatment
8. There are numerous problems with scientific study. So you cannot use the results of a study to train your clients?
Yes. But one of the basic steps in EBP is to critically analyze the study: If the study has methodological issues or has a different population than your client, you downgrade the evidence accordingly and lower your strength of recommendations.
9. Most of the studies in bodybuilding/strength training are on untrained individuals.
Yes. And rightly so, caution should be used when extrapolating recommandations to trained individuals. Exercise science is a relatively new field and studies in trained individuals are small in number, but accumulating. Generalizability (i.e. the ability to apply findings from a study to a given population) must always be taken into account when using research to guide decision-making.
10. I don’t care about “why” it works or the science behind. All I care about are results.
As previously mentioned, EBP evolved to get better results. It didn’t evolve to explain how or why a treatment works. There are 1000’s of life saving treatments and drugs where the underlying mechanism(s) are just unknown.
11. Studies are looking at an average of the sample. There is a lot of individual differences.
Yes. In fact, n=1 studies occupy the top of the evidence hierarchy because it applies to the specific individual in question. But these are hard and almost impossible for certain outcomes like muscle growth or disease prevention. There are two concerns with so-called trial and error method that is often talked about.
12. The program worked for me!
What was the outcome measure? Strength, muscle growth, weight loss? What are you comparing against? Against your previous results? What was the magnitude of the benefit? Without knowing answers to these questions, the meaning of the word ‘worked’ is unclear.
Further, if it indeed worked, we still don’t know what made it work, or if it will work for someone else. So your personal anecdotes are often fraught with problems and unfortunately mean very little. And importantly, just because something “worked” doesn’t mean that another approach might not work better.
13. This X supplement was shown to increase muscle growth in an animal study. Should I use it?
Research in animal models is almost at the bottom of the evidence hierarchy. It is very weak and hence the uncertainty is high, and deserves no greater than a weak recommendation. Although animal models can serve an important purpose in preliminary research, evidence based practice should rely primarily on human studies when developing applied guidelines.
I saw a supplement study which showed a statistically significant weight loss. Can I use that supplement for my client?
No, you also have to look at how much weight the subjects lost. The term “significance” is a function of the probability of results occurring by random chance; it is not necessarily related to the magnitude of the effect. Provided a large enough sample size, results of a study can be statistically significant even with just a 1 lb weight loss over a 1 year period. This is known as ‘clinical significance’.
Would you take a supplement to lose 1 lb in a year? Depending on the cost, the burden of taking a pill every day, and how much you value weight loss, you may or may not.
14. EBP does not consider a science-based approach.
EBP does consider a science-based approach. A science-based approach provides strong evidence when the program or treatment violates fundamental principles or universal laws. For example, homeopathy.
However, EBP does not support evidence just based on biological plausibility or mechanistic evidence. For example, if a new diet tells you to eat as much as you want to lose weight, it goes against fundamental laws of thermodynamics. You do not need an RCT to make strong recommendations against this diet
15. “This house believes that in the absence of research evidence, an intervention should not be used” This was the motion of a debate which took place at the end of the recent PhysioUK2015 Conference in Liverpool.
As you know by now, EBP does not rely on RCT’s. To quote the famous saying in EBP: “There is always evidence”. It is an unfortunate misrepresentation of EBP/EBM to assume that without RCT’s, a treatment cannot be recommended. For example, smoking has perhaps the greatest detrimental effect on health of any social habit, and health-based organizations universally recommended against its use. But we do not even have even a single RCT on smoking!
Effects of smoking are from observational studies. But since the magnitude of harm is very high, it upgraded in the evidence pyramid. Once again, this shows why the hierarchy is not set in stone.
16.‘Parachute use to prevent death and major trauma related to gravitational challenge’. This is the title of the paper published in BMJ. The paper satirically argues that parachute use has not been subjected to rigorous evaluation by using RCTs’ and therefore has not been shown to save lives. Critics of EBP have used this as a criticism of EBP and the reliance of RCT’s.
EBP has always maintained that RCT’s are not required when the magnitude of benefits is very high.
For example, insulin injection for diabetes, Heimlich maneuver, and anesthesia are all examples of treatments where the magnitude of benefit is very high, and hence RCT’s are not required nor asked for.
17. I do not have enough knowledge to critically analyze studies.
There are a few resources in the field of exercise and nutrition that critically appraises the evidence for you. They are www.alanaragon.com, www.strengthandconditioningresearch.com, www.weightology.net.
In closing, we hope the article has helped you better appreciate and understand this simple framework called evidence based practice or evidence based medicine. EBP is currently the best approach we have to make decisions related to health, fitness or strength and conditioning.
A good EBP practitioner should have a strong understanding of both the practical and the scientific aspects of exercise and nutrition; and more importantly, an untiring commitment and empathy to your clients and their values and preferences.
Related Articles
What is a P Value?
December 31 2016
P value is one of the most important values in research, yet it is a challenging concept to understand. In this article, I am taking an intuitive approach using a weight loss example to explain the concept of p-value. Of course, I have omitted the details and technical terms to focus on the big picture. So here we go:
What is really a p-value?
P-value: P-value or probability value is arguably the most important value in science. Believe it or not, approval of drugs worth millions (maybe billions) of dollars or treatments that can save thousands of people finally comes down to this little p-value. You can usually find them in the abstract or the result section of a study
The picture below shows the result of the famous study by Doll and Hill in 1956. The study showed that smoking indeed causes lung cancer thereby saving millions of lives.
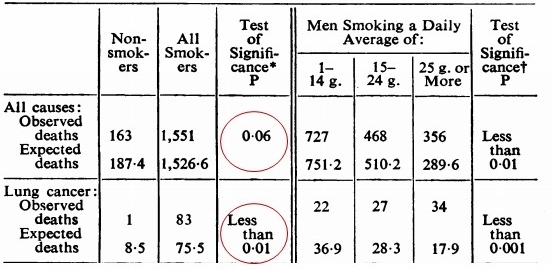
Why do we need a p-value?
Since now you know the importance of a p-value, why do we really need it??
Sample Study: Let’s take an example study where a researcher wants to know the average weight of the inhabitants of the planet Mars. Let’s imagine that the total population of this planet consist of 10 people and the average weight of the population is 150lbs.
He randomly selects a sample of 3 people.
1. He gets an average of 137lbs. And he proclaims that the average weight of the population in Mars is 137 lbs.
2. Now just to confirm his initial study, he takes another 3 people from the population of 10. Guess what, now he gets an average value of 140lbs.
3. He takes yet another sample of 3 people randomly. Now he gets a value of 147lbs. Now the researcher is really confused. Why are we getting different numbers? Is science broke?
Sampling error: These different or ‘wandering’ numbers are due to selecting different samples from the population. And hence called sampling error. Error in latin means “to wander”. So the question is how can we confidently say that the result of any study is due to our intervention and not due to sampling error. Or, in other words, how can we say it not due to ‘chance’?
And this is exactly why we need the p-value:We want to know if our results are due to the intervention or due to these sampling errors or ‘chance’. In short, p-value is way to tackle the problem of the sampling errors when you are trying to infer something about a population. So anytime you hear P value, think about sampling error.
So how does this p-value work?
Now here comes the million-dollar question; but how on earth does the p-value ever know when the results are due to sampling error or the intervention?
Let’s take a personal weight loss scenario: Imagine you are trying to lose weight on a new diet. One morning you step on the scale and the scale says you lost 1lb (164lbs) and you just carry on with your daily stuff. A few weeks later you step on the scale and now it shows you lost 2lbs (163lb) and you carry on with your daily routine. A few weeks later, you step on the scale and now you have lost 5 lbs (160lb)!! Wow…all of a sudden you are so excited and you tell all your friends and people at work that the weight loss diet works!
Now the question is why were you so excited about the 5 lb loss, but did not give a damn about the 1-2lbs loss? Why? Why? The answer is you are using your own ‘P-value’ or probability by comparing your weight loss numbers to a personal distribution graph that you carry in your head. So what is this personal distribution graph?
Personal distribution graph: This personal distribution graph reflects the probability of your typical weight fluctuations in your adult life. As shown, it could be weight gain or weight loss. There are three main points to this graph that is very important to keep in mind.
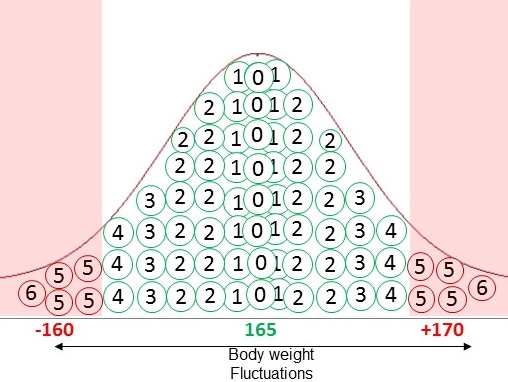
Now back to our 5 lb loss. Since the weight loss of 5lb falls in the tail end or the low probability area of the curve, you know that the probably of getting the results due to chance (means water weight, missing meal, being sick) is low. Hence you are convinced your results are due to the diet and therefore rightfully excited. On the other hand, if the weight loss was 2-3 lbs, it will be in the middle of the graph or in the high probability area. And since it in the high probability area, you know there is a high probability or high likelihood that the 2-3lb weight loss is due to errors like water weight, measurement error, skipping a meal and so forth or chance. In fact, this is exactly how the concept of p-value works. The probability value here is simply the P-value.
What about studies?
Wait… but in studies, the p-value is the probably of the results due to sampling errors, right? How do we get a graph of sampling errors?
Study distribution graph: Yes, in a study, instead of a personal distribution graph, we have a study distribution graph. Unlike the individual weight changes in the personal distribution, each circle represents the average weight of a random sample. And place of errors due to water weight, skipping a meal and so forth, here the errors are due to selecting different samples, namely sampling errors. Remember the section we talked about the study about weight of the people in Mars?
And guess what? Just like your personal graphs, there is a high probability area and low probability area in the study distribution graph. The tail end of the curve or the low probability area represents probability of 5%. So anytime your results are on the tail area, we know the probability is less than 5%.
Now just like the personal distribution graph, if the study results fall on the tail end or the low probability area of the curve, we know that the probability value or p-value is less than 5%. That is, the probability of results being due to chance, in this case sampling error, is very low. Hence, we say that the weight loss is due to the diet or the drug or the intervention. Or we say the results are statistically significant. And that is all there is to know about the P-value.
Now for a few commonly asked questions:
You can skip this section if you desire to:
1. How do we get the study or sample distribution in a study?
Good question. The official name of this graph is the “sampling distribution” since it represents the “sampling errors”. As you know by now, if it weren’t for this graph, there is no way we can find the p-value.
Imagine the weight loss study we talked about where the researcher takes 3 random people out of a population of 10. Theoretically if he takes 100’s of random samples of 3 subjects, we will get a curve which looks exactly like the personal distribution graph with high and low probability area. Now all we need is the distance between the middle region and the tail area, right?
To get the distance, we use the only two information available to us; the average of our sample and the number of subjects or sample size. Plugging these into an equation and using certain statistical assumptions, we get the distance. The catch here is that as the sample size increases, the distance between the middle region and the tail area gets shorter. Hence, it becomes easier for our result to fall on the tail area with larger sample sizes. Sp P-value depends on the magnitude of our result AND our sample size.
2. Ok. Why did you choose 5% as the cut off and not 10%? And how on earth do you know the tail area is 5% probability?
Glad that you asked. The 5% is an arbitrary cut-off. We still use it because of of the force of convention than anything else. In some fields, like particle physics the threshold is .003.
If we graph physical measurements, like height, blood pressure in 1000’s of people, the graph will look like a bell curve (looks like a bell). And some very smart people have calculated that 95% of the values will fall in the middle area and 5% falls on the tail area. That’s how we know the tail area gives us 5% of the probability.
3. The actual definition of the p-value says”, The P value is the probability of getting the results you did (or more extreme results) when the null hypothesis is true. What is the null hypothesis and why do we need it?
A null (means zero) hypothesis means that we are hypothesizing that there is zero or no difference between our two groups (for example weight loss drug and control group). In fact, we do a study because we think there is a difference between the two groups and want to show there is a difference. So stating the null assumption prior the study is a bit weird.
Now why do we need this weird assumption in the definition? Remember, the 1st important point in personal weight loss example: My personal distribution is my typical weight fluctuations when I am NOT trying to lose weight or when I am NOT on a diet. If the graph included the weight lost due to the diet, you have no clue whether the 5 lb is due to the water weight, measurement error or due to the diet, right? Hence the p-value totally depends on this assumption of null hypothesis.
4. So is p-value the probability of getting the results due to ‘chance’?
Strictly speaking, nope. All we did was we just took the 5lb loss and superimposed on our personal distribution graph. The result of 5lb we got could still be 100% due to chance. A great analogy is winning the lottery ticket: Although winning a lottery is extremely unlikely and would fit nicely in the tail area or the low probability area of our distribution, none will dare to to say that he/she won the lottery due to trickery and not due to chance because the p value is less than 5%, right?
5.. So if the p-value is less than 5%, we can say the results are credible?
Always keep in mind that the p-value is a measure of the sampling error or just a measure of statistical uncertainty. Hence the reason when it is low, we call the results ‘statistically’ significant or ‘statistically’ important
The study could have very low p-value, but it could be still biased if the methodology sucks, the instruments used are not valid, there is no randomization, no blinded testers and so forth. Unfortunately, people love to ignore these problems and just blindly focus on the p-value.
Conclusions
I really hope you have a better understanding of the p-value after reading the article. I have omitted the details, like standard error/deviation, alternate hypothesis, normal curve and such and just focused on the big picture. I do think without the personal weight loss example it is quite hard to grasp the concept. And I have read almost every other statistical approach/book to explain p-value.
Next time, when someone talks about a p value, 1) Try to picture the personal or study distribution when the drug or the intervention has NO effect 2) and now superimpose the study results on this graph. 3) If the results fall in the tail area or the low probability area, then p-value is below 5%, and the study is ‘statistically significant’.
Wishing all my Exercise Biology readers a wonderful 2017!
Related Articles

How to Check the Quality of a Research Article
November 25 2016
This is one of the most important aspects of a research study, yet the most overlooked or ignored by researchers and readers. If you read studies or believe in science, keep reading:
Why is study quality important?

Photo Credit: Evandro Inetti/ZUMA and Tischenko Irina/Shutterstock
However, if the study does not adhere to appropriate methods to minimize bias, even an RCT is only as good as an opinion piece in Muscle & Fitness. Or maybe I should just say an article in M & F.
How do you assess quality?
There are three major methodological characteristics that you should look for to assess the quality of an RCT.
There are other ones like Intention-to-Treat ( ITT) and such. But the above mentioned ones have shown in studies to over exaggerate the benefits by almost 40%. That means, if a study lacked concealed allocation, a strength increase up to 40% could be just due to bias.
What about my studies?
Nobody is saying researchers cheat or commit fraud, but these things happen subconsciously even if you have the best intentions. That includes myself as well. I still cannot believe journals, even top journals, accepting papers which had no blinding of testers.
Why there is a replication crisis in science
Conclusions
Thank you for reading Exercise Biology.
Related Articles
Over 50? Start Power Training
August 25 2016
We have all heard about circuit training, functional training, HIT training and so forth. But what about power training?
Power training simply means moving the weights as fast as you can and lowering it under control during the lengthening phase. Or in layman’s term, you lift the weights fast and lower it under control. It is also called as high velocity training.
Here is a video of one of my subject performing power training on a pneumatic chest press machine:
Why folks over 50 should do power training?
What is power: Strength is the ability of muscles to produce force, whereas power is the ability to produce force quickly or rapidly. Speaking mathematically, muscle power is the product of force and velocity.
Like it or not, there is a steady decline in physically function as we get older. And this decline in function is largely attributed to the declines in strength.
Power vs Strength: Guess what? Recent studies are showing that muscle power may be slightly more important than strength.
Is Power Training better than conventional resistance training?
The first question is whether power training is actually better to improve power?
In fact, power training is now studied even in Parkinson’s patients, multiple sclerosis, osteoarthritis, and in mobility limited older adults.
Do I need any special equipment for power training?
Nope. Power training studies have used bodyweight, elastic bands, weighted vests, pneumatic machines and standard plate machines. So all you need is a willingness to embrace science.
What loads should I use?
Most studies have used loads ranging from 50% to 70% of 1RM. There is some evidence that points to lighter loads to improve activities such as walking and balance, while heavier loads may favor activities that are more force dependent, such as chair stands and stair climb. But evidence is currently lacking
What about safety?
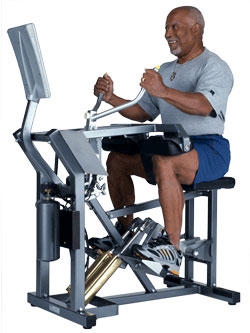
What about the quality of studies?
Conclusions
Reference 1
Power training using pneumatic machines vs. plate-loaded machines to improve muscle power in older adults.
Related Articles

Can exercise prevent the decline in physical function in older adults?
May 25 2015
This is the largest and longest exercise study ever conducted to find out if exercise can prevent disability in older adults.

Why is physical function important in older folks?
Physical Function: What is physical function? It is the ability to carry out daily activities that require physical ability, ranging from self-care (basic activities of daily living (ADL)) to more-vigorous activities like carrying groceries, walking up the stairs and so forth. When the functional decline is severe ( termed disability), that is when you have no choice but to depend on others/ end up in a nursing home/or in bed. So physical function is a major determinant of quality of life in the elderly.
Muscle Mass Decline: Now guess what, decline in muscle mass and strength is largely responsible for the decline in physical function with age. As you get older (> 50), like it or not, there is a steady decline in muscle mass (1-2% per year) and strength (called sarcopenia).
Why was the study done?
Exercise & Function: The study was done to find out if exercise as claimed can prevent the onset of physical disability, especially walking disability (walking 400 m).
Previous Studies: Almost all the exercise studies were short-term and measured intermediates such as strength and muscle. The effect of exercise on long-term disability is unknown. It is unknown if frail older adults can keep exercising regularly and/or older adults who have multiple diseases can adapt well. It is the difference between a 12-week and a 3-year weight loss study
What were the methods?
1635 Men and women aged 70 to 89 years, and who are at risk of disability (vulnerable folks), were randomly assigned to two groups. Subjects were recruited from 8 different centers in US.
The outcome measure is the failure to walk 400 meter in less than 15 minutes (also called walking disability or mobility disabilty).
What were the results?
In the exercise group, walking disability was seen 30%. Whereas in the control group, they observed a higher number of disabilities (296 or 35.5%).
In other words, there was a (5%) reduction in disability in high-risk older adults with exercise.
My Comments:
Physical function, Quality of Life & exercise: I have a Master’s in this field, worked as trainer for more than 10 years, ran a university fitness center for 4 years, and now doing my Ph.D. I have preached endlessly about the benefits of exercise when to comes to cancer, heart disease, obesity, diabetes and cognition to people. But I have never really given a thought about exercise to improve physical function in elderly until I saw my Mom’s struggle with cancer. She never really worried about dying, all she wanted was to do the basic things in her life without needing others help. And that affected her quality of the life the most.
In fact, research always focused on death as an endpoint since it is quantifiable and objective; quality of life on the other hand is qualitative and subjective and was less of a concern. Recently the concept of active life expectancy- the average number of years of life free from disability- has slowly come into picture. NY best-selling author Atul Gawande’s recent book “Being Mortal” talks about how in the mad race to make people live longer we forget how well they live those last years.
If you think about it, there is a pill for every major disease and people are living longer and longer. But, guess what, there is no medicine out there to reduce or prevent the decline in physical function in adults. The only option we have to slow the decline is exercise. Reducing the decline in physical function and thereby improving quality of life is probably one of the most important benefits of exercise and the one which is overlooked the most.
Healthy Participant bias: If you recruit subjects for an elderly study, the majority who show up for the study will be above average in health. The people who are in bad shape and need help are the ones struggling at home, not able to drive or walk around because of health issues (physical, cognitive, hearing, vision etc) and won’t see or able to read your study flier. This is called the healthy participant bias. This is the reason why all journals insist on reporting the recruitment protocols and why we shouldn’t skip reading those. The current study hence had a screening process and only recruited subjects who had lower physical function than average.
Osteoporosis: When I started r research in this area, I always wondered how come everyone knows about osteoporosis (loss of bone), but nobody really knows about the term sarcopenia (loss of muscle mass and strength). Loss of ,muscle mass and strength can lead to decline in physical function and falls, and is probably more important than osteoporosis. A large part of the reason FDA is still hesitant or slow in approving treatments or drugs is due to the lack of a consensus definition of sarcopenia. We still don’t know what is the cut-off point where loss of muscle starts to show up as decreased function. In fact, decrease in muscle and strength is not a good enough reason for pharmaceutical and regulatory agencies to approve drugs. This is similar to the development of drugs in osteoporosis; the drugs had to show a decrease in bone fracture risk than just increase in bone density.
Exercise Intervention: What was the specific exercise intervention used in the study?
- 30 minutes of walking at moderate intensity adding upto 150 min/week
- 10 minutes of primarily lower extremity strength training by means of ankle weights (2 sets of 10 reps),
- 10 minutes of balance training & large muscle group flexibility exercises.
-The intervention included attendance at 2 center-based visits per week and home-based activity 3 to 4 times per week for the duration of the study.
5% decrease means what: Now what really does a 5.4% decrease really mean? Does it mean you only get 5% of the disability or what? A large part of evidence based approach is communicating risk to the lay person so they can interpret and apply the evidence. A better way to convey risk is through numbers needed to treat (NNT). So a 5% decrease means you have to treat 19 people with exercise to prevent one case of disability in 2.5 years ( 19:1)
To give an example, aspirin is commonly used to prevent heart attacks. The NNT for aspirin is 1667 for cardiovascular problems. This means you have to treat 1667 people to prevent one cardiac problem annually. Now you can clearly see the uncertainty of taking a pill. You can also find out how many number of people get harmed using NNH (Number needed to harm). For example the NNH for apsirin for bleeding is 1: 3300. Next time the doc prescribes you a drug, ask for the NNT’s and NNH’s.
Conclusions.
Related Articles
Are low reps or high reps better for muscle growth in trained lifters?
October 01 2014
If you are a trained lifter, are high reps (8-12) reps better for muscle growth ? Or should you do low reps ( 4-6 reps) to increase a muscle growth? This was the exact question raised in a recent study.
What was the purpose of the study?
Though 8-12 repetitions are universally regarded as the optimal range for muscle growth, there is very little evidence that show any advantage of high reps (8-12) over low reps (4-6 reps). The few studies that did compare low reps to high reps suffered from 2 major problems:

Unequal Volume: The volume wasn’t same for both groups The 8-12 rep groups always did more volume than the low rep group. For example, one of the studies quoted in the paper showed an increase in muscle growth with high reps. To my knowledge, this is the only study that showed an advantage of high reps over low reps. The bodybuilding group did 9 sets of 8 - 15 reps (40-80% of 1RM). Now guess what the powerlifting group did? 5 sets of 3 reps (90% of !RM). So the volume of the bodybuilding group did almost 5 times more volume than the powerlifting group. The second study that showed identical results as reported in the paper is the exact same study, but reporting other variables. What about studies which did equate volume? The studies which did equate volume found no difference between high rep and low reps in muscle growth.
Not Trained: All the studies above used untrained subjects. In untrained subjects, everything works. In trained subjects, the muscles are less responsive.
Hence it is a great question to ask whether lower reps (or heavier load) performed at the same volume as high reps (or lower weight) could induce greater muscle growth in trained folks. And this is exactly the question the researchers asked in the current study. as mentioned in the paper, it is just a comparison of a powerlifting routine to a bodybuilding routine with similar volumes . To put it another way, is it the pump (high reps) that matters or is it the high load (low reps) that matters in muscle growth? Let’s see.
What was the study design?
Study Design: 17 well-trained subjects were randomly assigned to two groups. After 8 weeks, there were 9 in the bodybuilding type or high rep group, and 8 in the powerlifting group/low reps groups. The subjects’ experience ranged from 1 to 10 years in weight training.
Low Rep group: Hit one muscle 3 times per week
Sets * Reps : 7 sets of 3 reps
Rest between sets: 3 min
All sets to failure
90 minutes/workout
High Rep group: Hit one muscle 1 time per week
Sets * Reps: 3 sets of 10
Rest between sets: 1.30 min
All sets to failure
17 minutes/workout
As you can see, the volume was equalized by using Load*Reps*Sets. So for example, for the chest muscles, the low rep group did 63 reps while the high rep group did 90 reps.
How did they run the statistical analysis?
If you don’t care about the stats, you can skip this part. In my understanding, there are two common ways to analyze the results of a study:
Post Test: You can just simply look at the difference between post test results in both the groups. That being said, if the groups were different at the beginning of the study, the final results will be influenced by these differences. Even if you conduct the prefect randomization with a large sample size, chances are that the groups will be slightly imbalanced in the beginning. The group which had a higher average will tend to have a lower score, and the group which started lower will tend to have higher scores by the end of the study. This statistical phenomenon is called regression to the mean.
Change Score: Or you can take the difference from pre-test to post-test in both groups and calculate the difference to obtain the gain score or change score. Here, since we are including measurements twice -pre test and post-test, you are adding up errors unless the test are highly reliable. In addition, the regression to the mean will have an influence here too.
So what is the solution? Basically computing just one value for the pre-test for both groups. This would look like both groups started out with the same score in the beginning. This is usually referred as baseline adjusted scores or adjusted scores.. So now we can just compare the post test results without worrying about the nasty regression to the mean. This type of analysis is not very common. However, it is frequently used in drug trials and generally considered to be the best method to maximize statistical power in a two group pre-post design. So the researchers did an excellent job with statistical analysis.
What were the results?
Muscle growth: No differences were seen between the groups for biceps thickness. Both groups improved by around 13%.
Strength: For bench press, the low rep group had a 13% increase, while the high rep group had a 9% increase. For squats, the low rep group improved 26%, whereas the high rep group improved 22%. This is after the adjustment as I wrote in the analysis. The numbers shown in the table are the non-adjusted values and hence the percentages will be different if you calculated using those numbers
Conclusion: Though there was little difference in muscle growth, considering the time (90 min vs 17 min), high fatigue and injuries (2 injuries) in the high load group, the high reps or bodybuilding type of workout appears to be more suited for muscle growth.
My comments
Low reps vs high reps: The topic of low reps and high reps has always fascinated me. In fact, this was the exact question for my Master’s thesis in 2005. I used beginners, but the concept was pretty similar of equalizing time under tension in both the groups. Also, my first ever online article in 2006 was about repetition range and hypertrophy. My hypothesis was that low reps would have a greater hypertrophy than high reps if the volume was equalized. However, after all these years of reading the literature, the less and less I am convinced that there is a great difference between low reps and high reps to talk about. The last article I wrote on high reps and low reps in 2010 was based on a study which showed that there is a limit to protein synthesis, and there is no difference in protein synthesis with high reps and low reps. Apparently, the conclusions I wrote in that article were almost identical to the current study. That being said, that study was done in untrained lifters. I even had a graph to show how this may turn out in trained lifters. So I have been waiting for all these years for a study on trained lifters comparing repetition ranges and looking at actual muscle growth.
8-12 reps: So if there is no direct study to show that 8-12 reps are optimal for muscle growth, how come bodybuilders always used 8-12 reps? I think this is a good example of how we tend to confuse cause and effect in anecdotal observations. In my opinion, anecdotally, 8-12 reps are considered “optimal” for muscle growth not because it is optimal for muscle growth per se, but for reasons that have very little to do with actual muscle growth and more to do with feasibility, recovery and injury concerns.
We all know low reps cause greater fatigue and hence can impair recovery. Also, as the individual gets stronger, the heavier weight that comes with low reps can be very hard on joints often leading to joints aches and injury concerns. Now what about the practicality of low reps? What do you think is really practical in your gym? Doing 7 sets of 5 of bench press with 3- 5 minute rest, or 3 sets of 12 reps with 1 -2 min rest (35 reps vs 36 reps)? All the above concerns become very real when you are in the gym almost every day for years like a typical bodybuilder. Consequently, bodybuilders naturally gravitated towards high reps. What about powerlifters? Power lifters have no choice but to perform low reps because their sport demands low reps. And hence they have to extensively rely on load cycling, deloading, not going to failure and other strategies to minimize fatigue and stay injury-free. So 8-12 reps for muscle growth was born more out of necessity than choice, and for reasons not directly related to actual muscle growth as most people think. So there is no magic in high reps, I think.
This is the large reason why there is efficacy and effectiveness trials. Most of the studies in exercise physiology are efficacy trials: Trials which are done under ideal or controlled conditions. All these problems outlined above will not be evident or will be missed in a 8 or 10 week controlled lab study, which is primarily designed to look at muscle growth. On the other hand, effectiveness trials are trials trying to simulate the real world. In effectiveness trials, one of the primary questions is whether the protocol or workout program is actually feasible in real world conditions. So even if efficacy trials show muscle growth is more with a certain rep range, effectiveness trials may show something totally different.
Volume: At least from my perspective, the simple question is if you do 1 sets of 12 reps, can you get greater hypertrophy with 2 sets of 6 reps? Here, the time under tension for both the groups is the exact same: 12 reps. So the comparison here is just between load, which is almost double in low reps, and metabolic fatigue, which is very high for high reps and very low for high reps . I am guessing the choice of 3 reps than 5 or 6 reps was to avoid any sort of metabolic fatigue in the low rep group. In the current study, equated for volume, the TUT for low reps was 63 reps and high reps was 90 reps. Will equalizing the TUT make a difference? I don’t know. Is that practical? Maybe not.
Sample size: Sample size is obviously small. There are two schools of thought when it comes to sample size: One school of thought is that even if it is a small sample size, you should conduct the study and publish it. And in the future, a meta-analysis can pool all the small studies to come up with a large sample size. The other school of thought is that you shouldn’t embark on a study when you clearly know you won’t be able to recruit enough subjects to find a statistically significant difference. I favor the former. In fact, the study which I recently conducted had 9 and 8 subjects in each group. But the criteria for recruitment was very narrow and hence very hard to get subjects. In fields like exercise physiology, it is not practical to conduct large scale multi-center trials or hope to receive NIH grants that give you a couple of million dollars every few years.
Failure: This is one area I felt the researchers could have been done a little bit differently. For example, the low rep group performed 7 sets of 3 to failure for a body part 3 days a week. This is very taxing on your nervous system and muscles, and is evident from the subjective reports and injuries sustained in the low rep group. If ‘going to failure’ is an integral part of bodybuilding, ‘not going to failure’ is an integral part of power lifting. I would have been very happy if they had at least instructed the low rep group to stop one rep shy of failure. And this change would have made the routine more comparable to a typical powerlifting routine. I talked to Brad about it. Could the heavy load taken to failure affected recovery and thereby muscle gains? I don’t know. As is typical of Brad, he calmly acknowledged it and said it probably won’t make a big difference since they maintained strength levels and even gained some. I agree with Brad to a certain extent.
Strength: As expected, the low reps group gained more strength than high rep, especially in the squat. But strength is traditionally defined as the maximum amount of weight you can lift for one repetition or 1 RM. I would have loved to know what the 10 RM for each group was. My guess is that the high rep group would improve the 10 RM more than the low reps. As dictated by the specificity theory, the neural adaptations inherent to low reps are inherent to low reps and is less unlikely to transfer to high reps. And if it is true, I don’t see a logic for bodybuilding routines to include low reps to increase muscle strength and thus muscle growth. For a bodybuilder, what you need to worry about is the maximum amount of weight that you can do for 8 to 12 reps and not 1 repetition.
Now how to better analyze the results?
Typically, almost all studies are analyzed based on the p-value. Here is how to do it using confidence intervals.
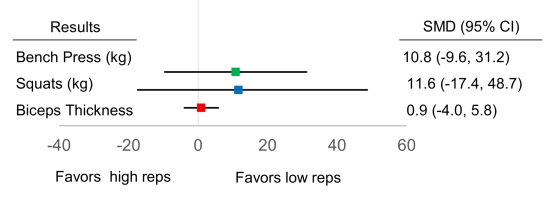
The horizontal line says that we can be 95% confident that the true mean difference between the groups will fall somewhere on that line. For example, as you can see in the figure, the difference between the groups (mean difference) for bench press in the current study is 11 kg (10.8) in favor of the strength training group. And if we repeat the study a number of times, we can be 95% confident that it could fall somewhere between 10kg in favor of the high rep group, or 31 kg in favor of the low rep group as shown by the upper and lower limit. This interval is called the 95% confidence interval (CI). Now you will admit that it is a bit too wide of an interval to make any definitive conclusions about whether to use high reps or low reps to increase bench press. So how the can you make the line or the interval shorter?
Now here is where our sample size comes in. The greater the sample size, the shorter the horizontal line of our interval, and thus greater our confidence or certainty or precision. Here, even though the confidence intervals are pretty wide for bench press, we clearly see that there could be a large benefit as the upper limit possible for bench press approaches 31 kg and 10 kg. If I am coach or a lifter, these are huge numbers. So we might very well embark on a future study with a larger sample size to see which group is really better. Now if the upper limit was pretty small, for example 3-5 kg for bench press, I wouldn’t bother conducting a future study to see if high reps or low reps are better.
Now if we used p values, let’s see our how our interpretation goes: Since the horizontal lines cross the vertical line of no difference (P > 0.05), there is no statistically significant difference between the groups. Hence we conclude that there is no benefit of using low reps or high reps for bench press. There is no further interpretation or discussion of the study results. Apparently, both the p-value and confidence intervals are calculated using the same method , but the interpretations and conclusions we reach are very different.
There is more to it, but I hope this gives an introduction to the benefit of using CI to interpret and report results.
Note: I used the non-adjusted values since the baseline adjusted values were not shown the paper. After the baseline adjustments in the current study, the squats horizontal line favored low reps (did not cross the vertical line of no difference)
So what does 13% increase in bicep thickness mean?
Now, we all know what a 5lb or a 10lb increase in bench press or squat means. We all know what a 1/4 in or half inch increase in our biceps means. But what does a 13% increase in biceps thickness using ultrasound means?. Even if you showed a 13% increase in muscle thickness, you may not notice any difference looking in the mirror or using a tape measure. It maybe very meaningful if you are a bodybuilder on stage at 5% body fat under a row of bright lights. Finally, what counts is whether your muscles ‘look’ big. The same goes for measuring muscle size using MRI. This is usually called the practical or clinical significance. It would be good to know how this percentage translates to a tape measure reading.
Blah blah.. so should I do high reps or low reps?
In my opinion, this is one of those questions which will be debated for years. And this has more to do with our human nature and cognitive biases and less to do with the science. Things will never be black and white, but as humans we favor certainty and tend to be very uncomfortable with ambiguity. If you notice, this is one reason why a lot of quacks thrive; they always make absolute claims and people ‘subconsciously’ tend to love anyone who can take complex issues and simply portray it as black and white. Mind you, research can never eliminate uncertainty, it can only minimize it.
Now instead of worrying about doing low OR high reps, why not just do both:
There are many other options, but you get the point.
Brad Schoenfeld: Brad is the lead author of the study. Brad is one of those who is single-handedly changing the field of hypertrophy. This study is a perfect example of how he investigates questions that people have been asking for years, but no one ever bothered to conduct a study on. It is certainly a mark of a good researcher. What I really like about Brad is his passion for the field of hypertrophy and towards a scientific approach. Every time I talk to Brad, in person or on phone, we just wallow in science and theories with the same enthusiasm and amusement shown by two little kids playing outside in the rain. I am in school now and teach a bit, but I am yet to see a student that shows that hunger or desire to learn more and excel in their field. And this is exactly what is common to all those big names in the fitness field, like Lyle Mcdonald, Bret Contreras, Nick Tummenello, Alan Aragon to name a few (all science-based too).
Conclusions
I think that’s all I have. I know it is a bit long, but I hope you learned a little bit about research and muscle growth after reading it. Thank you for reading.
Reference: Effects of different volume-equated resistance training loading strategies on muscular adaptations in well-trained men
Related Articles


What should fitness professionals understand about pain and injury?
January 08 2014
I wrote an article a couple of years back to introduce fitness professionals to the new revolution in the understanding and treatment of pain. Despite making some progress forward, I think there still remains some confusion and misunderstanding about the relationship between pain and injury. It goes without saying that pain is a topic that fitness professionals should have a better understanding. I have tried to include a few questions that I feel trainers and strength coaches might have trouble with. So without further ado, here we go:

What is this whole talk about how injury and pain are not related and how pain is in the brain? Is it true? If so, I don’t get it.
We used to believe (some people still do) pain and injury to be highly correlated and would utilize the measure of pain as an indicator of tissue damage. Unfortunately, as we begin to learn more about pain and injury, it is clear that pain is not an accurate indicator of injury nor damage. To understand this better, we have to understand a very important concept. So pay attention.
Pain does not (technically) begin at the level of the tissues: While we once thought pain to originate at the level of the tissue (and that “pain” information was carried up to the brain), we now understand that these carriers, nociceptors, relay “danger” information to the brain for processing. . Once the “danger” information reaches the brain, it is then up to the brain to decide whether these signals are dangerous enough to respond by producing an output of pain. So we don’t have pain receptors or ascending pain pathways as we commonly thought. Pain doesn’t begin until the brain determines it is needed.
It is crucial that we understand this response is quite individual. One may have a very serious injury and complain of little to no pain, while another may have a very minor injury and experience extreme pain. The degree of injury is not always related to the degree of pain. Hence they say, injury and pain are not related and ‘pain is in the brain’.
But what makes the brain think it is indeed threatening or I am in danger, and let’s generate some pain?
Well, many things, actually. Your attitudes, beliefs, past experiences, knowledge, social context, sensory cues, nociception and so forth may all be confounding variables influencing your brains decision. What we have to understand is nociception is just only one of many inputs that the brain assesses to see if it is indeed in danger. Pain is only generated if the brain concludes that body is in danger and action is required.
This is bull crap; are you telling me if I cut my hand, I won’t feel pain? .
A lot of people who are resistant to accepting this concept may only be considering examples where they had injury and then felt pain. A=B. Unfortunately, this relationship isn’t as clear as we may think. We may be subconsciously ignoring the countless times where we had an injury and felt no pain (or pain not proportional to the extent the injury). We have experienced plenty of bruises and cuts, with little clue on how or when it happened.
Forget the tiny bruises and cuts. It is well known that around 40% of the people admitted to the emergency room with horrific wounds have no pain, and in some, no or low pain even after long delays (1). And mind you, these people are alert, rational and coherent (‘not in shock’ as most people tend to believe). If a crowbar is sticking through your neck or an amputed arm, doesn’t result in pain, why on earth would we think injury is an accurate indicator of pain?
So how could these horrific injuries result in NO pain? As we learned, nociceptors relay danger signals, and it is ultimately up to the brain to produce an output. Most often these horrific injuries happened in a context where survival of the person was at stake, which is a lot more threatening than the injury (ie. focus on the injury or sustain life). And as time goes by and the brain concludes that you are out of danger, it now focusses back on your amputated arm. I cannot work, I cannot lift my kids, I know and have seen amputees struggle, I can see the blood on the bandage: All these beliefs and attitudes and sensory cues are only heightening the fear or threat level of the injury in the brain. And guess what happens now? PAIN.
Now what if your thoughts/attitudes were more positive or less threatening? In 1950 Henry Beecher did a similar study. They wanted to see why soldiers who got injured in war took much less morphine than a civilian or why they had much less pain that expected. The results indicated that it is simply because of “meaning”. For a soldier, despite experiencing a major injury or an amputation, he still survived a war , and could return home and be with his family and friends. The soldiers beliefs and attitude was likely influential over the brains defensiveness, resulting in much less pain than expected (7).
And mind you, these things are happening in a split second and it is outside our conscious control. If you doubt such decisions can be made fast enough, look at the picture below. In fact, both the tables A & B are of the exact same length. Your eyes saw both the tables being the same length, but your brain perceived them being as different lengths in a nano second!
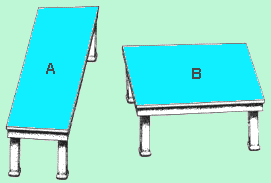
Again, I am writing all this to show that pain is not an accurate indicator of damage and brain constructs pain based on assessing all other inputs. Nociception happens to be just one of those many inputs.
If the brain sends an output of pain, and nociception is just one of the inputs, can we have pain without nociception?
Very good question and the answer is a big yes.
A classic example is phantom limb pain, which has puzzled us for years. In phantom limb pain, forget damage and nociception; people no longer have a body part, yet still feel pain (in their missing body part). Phantom limb pain is a remarkable example of how pain occurs with absence of nociception. We also see plenty of examples around us where people experience pain with no damage or injury.
Now how do researchers study these questions? Here are two popular studies:

As shown above, there are many evolving studies to demonstrate that pain can occur without any damage/nociception/injury.
I don’t care much about the science of acute pain from a cut or a wound. I have chronic low back pain for years due to the 2 herniated discs as shown in my MRI. How does all this brain talk ever change the treatment of chronic pain?
Since now we understood the biology of pain, it is a good time to talk about pain management. As you rightly pointed out, acute pain is pretty straight forward and well understood. As the name implies, it is just acute or short term. We get injured, we ‘may’ feel pain, healing takes over, pain goes away, and we are back to normal (usually 3-6 months). Nobody is really bothered about acute pain, what everyone is worried about is chronic pain.
Chronic pain has always been a mystery to us. Why should this pain last for years and years when injury had enough time to heal? Multiple bullet wounds and major amputations heal within months so why should this tiny injury to your knee or shoulder last for years and years? What do you say?
Or how come there are large numbers of people who have the same dysfunctional tissue but have no pain? We know that around 40% of the population have disc herniations but have no pain whatsoever. And guess what, these people do not end up in pain years later either. This is the exact reason why the American College of Physicians have come forward with clinical guidelines saying ”Clinicians should not routinely obtain imaging or other diagnostic tests in patients with nonspecific low back pain”. We now clearly know that abnormal findings on the x-ray and MRI ( like disc herniations, bulging disk, degenerating joints and so on) are clearly NOT related to the onset, severity, prognosis, or duration of low back pain. If 40% of the general population do have disc hernataions, I do suspect everyone who lifts weights will have one or two disc herniations. 3, 4
Before we understood the role of the brain in pain, we always thought that pain was an accurate indicator of damage and nociception equals pain. So chronic pain always meant that there is an injury yet to be healed. Hence all our treatments were focused on fixing tissue damage and dysfunctions (the biomechanical model). But now we know that in chronic pain, the injury has healed long back and what is maintaining the pain is the sensitive nervous system and the brain. Or in other words, the brain still thinks there is threat and hence still outputs pain.
So yes, all this brain talk has revolutionized the understanding and treatment of pain.
This is interesting, but what the heck do you mean by a sensitized nervous system?
Remember the last time you had a cut or a contusion? Not just the damaged area, but even the surrounding area was very painful even to the slightest of touch (defined as hyperalegisa and alloydynia). What we see here is an increased sensitivity of the nervous system. In other words, both the threshold for activation of the nociceptors is lowered AND the response of the nociceptors is increased. Remember that muscles, joints, skin are just the hardware, the nervous system is the software and where all the action happens.
Now In chronic pain, this nervous system sensitivity is still maintained. The brain believes there is a threat and hence rightly so sends an output of pain. So just flexing your low back with a small weight, which seemed pretty harmless, is now threatening enough to evoke pain.
So the simple goal of any pain treatment is to lower the sensitivity of the nervous system (includes brain).
I see. And how do you lower this sensitivity?
Two ways:
Top Down: Basically, means changing your attitude, beliefs, knowledge (neurophysiology of pain) about your pain and in turn, lowering the threat value of pain. People get hurt, they experience pain, healing follows, and they recover. But in some folks the pain lasts forever. And why is that? According to one of the most well-accepted models - the fear-avoidance belief model - people who have heightened fear of re-injury and pain are good candidates for chronic pain. Lack of knowledge or incorrect knowledge, beliefs ( hurt always means harm, my pain will increase with any activity and so forth), provocative diagnostic language and terminologies used by medical therapists like herniated disc, trigger points, muscle imbalance, and failed treatments can further heighten this fear or threat . So education to lower the threat is THE therapy here. We now have some very good evidence to show that just pain physiology education or the top-down approach is enough to lower pain and improve function 5.
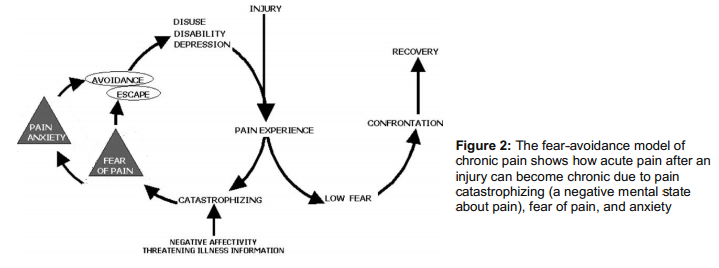
Bottom Up approach: The bottom-up approach is what we see around us: surgery, postural fixing, trigger point, muscle imbalance, movement re-education, manual therapy, acupuncture and the list keeps growing. Almost all treatments out there are trying to lower the nociceptive drive without much consideration to the top-down approach. This is solely because these treatments are based on the outdated model of pain. We now suspect that positive effects of manual therapy may be due to neural mechanisms than the tissue and joint pathology explanations that is often offered. So even the bottom up approach is working via de-sensitizing the nervous system. Although not intended, there are top-down mechanisms clearly at work even in bottom up approaches( like the placebo effect, a credible explanatory model, the belief in the therapist) .
So what we you need is a combined approach that takes into account the “entire individual” and that’s where the biopysycosocial model of pain treatments walks in. The bio psycho addresses the biology (nerves, muscle, joints), psychological ( beliefs, thoughts, fear) and social aspects (work, culture, & knowledge).
So what is wrong with some of the current treatments which are based on the old biomechanical model of pain?
As I wrote, they are just completely based on the bottom-up approach assuming tissue damage and nociception as the sole driver of pain. The is called the ‘find and fix it’ model.
A good question is if it is working, should we worry about all this brain talk?
It is estimated that 1 in 4 people in America are in chronic pain and this was 1 in 7 in the 90’s. So our approach was clearly not working (even if we thought it was). Furthermore, none of our treatments show any specific effects. That means for low back pain: manual therapy, acupuncture, general exercise all seem to elicit similar effects. 6
What is clearly disconcerting is these treatments are given in a context that there is something wrong with the tissues and we need to avoid/prevent /fix it. This structural pathology approach is great to raise the threat level in the brain and in turn maintain or worsen your pain. So even if you get pain relief, you may be nicely setting yourself up for some future pain problems.
Now I am confused. Should I tell people not to use an arched back when they lift because it can raise the threat in the brain? Should I stop foam rolling and other injury prevention methods?
Nope. Just like I wouldn’t advise anyone to cross the street with their eyes closed, I wouldn’t advise anyone to pick a 200 lbs barbell with a rounded back. The age-old simple advice of avoiding extreme loading at the end range of motion still holds good . So proper form is always recommended.
What we don’t want to do is overemphasize or exaggerate our case for injury and pain prevention. For example asking someone to sit with 20% tension in abs, always be upright and never slump, educating disc herniation means the end of the world, knees should never go past toes, spinal rotation is bad and so forth. If you don’t have any clear evidence and you are just speculating, and most are ,it is better to clip that ego and avoid the talk. You can do lot more harm than good.
Should you stop foam rolling and other injury prevention techniques? This is a good question, but a better question to ask is do these really prevent injuries in the first place? Most of the stuff that you often hear are just ‘claims’. If you think those really help, you have sufficient evidence and the client have injury concerns, then go ahead and do it. But what we have to be careful is the language we use to explain these techniques. For example, a better way to present foam rolling is to improve mobility and blood circulation instead of another tool to exorcise out those evil trigger points.
Can we prevent pain?
First, pain is a protective mechanism. If we didn’t have pain, we would be all dead. So pain is normal and necessary. Acute low back pain is as harmless as a common cold and is unavoidable in your life.
Second, what we need to worry about is pain that can become persistent or pain that sustains even after the tissue is healed. And the best way to prevent pain chronicity is to have a better knowledge of pain physiology and how pain is an output of the brain rather than a simple response to injury. It has been shown that people report less pain and less frequently after they receive pain education. Why? Simply because they have lowered the threat level in their brain. Pain education may also serve to lower the pain intensity with acute injuries. So throw away all those unnecessary fears and beliefs about pain and injury.
I am an NASM certified trainer. Our certification emphasizes a lot on postural correction and muscle imbalances. So what about posture?
As I wrote, almost all treatment modalities out there to explain chronic pain is based on the structure-pathology model. We have been studying and researching posture for more than 30 years and we still don’t have any evidence to show posture causes pain. In fact, we have very good evidence to show that posture is not correlated with pain. And If you have been keeping up with me so far, it is not so surprising. Is it?
What we have to understand is pain is just one part of a complex stress response. If you get injured, the body responds by releasing adrenaline, activating large muscle groups to evade threat, deactivating small postural and stabilizing muscles, changing your gait or posture to further avoid injury, slowing digestion, triggering swelling and inflammation and so forth. All makes perfect sense since the body wants to protect and escape from further threat or injury. Once the pain becomes chronic or threat becomes chronic, these complex protective responses are also maintained. You will still maintain those anatalgic or pain evasive postures, your core or postural muscles are still less activated, the over active muscles tend to shorten and become prone to trigger points, swelling and inflammation becomes wide spread and so on. So most of these responses that are often blamed for the cause of our pain are just the consequences of a well-designed, threat response system - posture just happened to be one of them.
I do some postural correction still, but don’t make so many claims as I used to. I just mainly do it for better aesthetics and to improve their function.
What about the strengthening muscles to relieve pain. I thought weak muscles were the problem. I had clients whose low back pain disappeared after doing low back exercises. How come?
Strengthening muscles may or may not have much of an impact on pain. What strengthening is good for is to raise the tissues tolerance, so that you don’t re-injure it. The pain relief people obtain when they do exercises could be very well explained by the non-specific effects of exercise. For example, you have managed to convince and comfort your client that movement is good and not to be feared, especially the body part in question. You also educated them that pain is due to weak or imbalanced muscles and will soon resolve. The improvement in blood flow, performing the actual movement (which was supposedly harmful), the self-belief that he or she will get better all contributes to lowering the threat value in the brain. If you care to notice, these top down and bottom up approaches are common to all movement or exercise based treatments. What is not common is the unique mechanism offered as the rationale for these treatments and their ignorance of the powerful non-specific effects of their treatment.
Once again, although the pain may resolve, we have used an explanatory model that is further instilling the belief that the pain is due to tissue pathology or tissue dysfunction or weakness. And that my friend is not good.
I think that’s all I have. I have omitted a few things, like the pain signature and other pain mechanisms which are a bit more complex. I expect (and hope) this article has raised enough curiosity in you to question some of your own beliefs and understanding about pain and injury.
Anoop.. you have made me really curious. So where can I read more about it?
Thanks!
Great sites to read:
www.somasimple.com (excellent forum)
www.bodyinmind.org
www.forwardthinkingpt.com
www.bboyscience.com
www.saveyourself.ca
www.bettermovement.org
www.thebodymechanic.ca
Great books to read:
Beginner Level
Explain Pain by David Butler & Lorimer Moseley (This is a must read)
Painful Yarns by Lorimer Moseley
Intermediate Level
Pain by Patrick Wall
The Challenge of Pain by Ronald Melzack
Sensitive Nervous System by David Butler
The Back Pain Revolution by Gordon Waddell
Topical Issues in Pain by Louis Gifford
Therapeutic Neuroscience Education: Teaching patents about pain by Adriaan Louw ( a book on how to do the top down approach)
Pain by Lorimer Moseley (DVD)
Acknowledgement:I would like to thank Jason Silvernail DPT, DSc, FAAOMPT and Joseph Brence, PT, DPT, FAAOMPT, COMT, DACc for helping me edit the article. Special thanks to Joe for painstakingly going through the article and making sure everything I wrote is accurate and consistent with the pain science. Please do bookmark his excellent website: www.forwardthinkingPT.com
Please do share this article to everyone you know. It is probably one of the most important articles I ever wrote, and that you will ever read.
Related Articles


Studies are conflicting so I don’t believe in scientific studies
October 11 2013
The is one of the most common arguments against an evidence based approach or scientific approach. I have lost count of the times I have read comments on facebook and forums that reads ‘one study might say it helps while another might say it doesn’t’ or ‘you can always find a study which agrees with your position’. Hence a scientific discussion based on studies is worthless.

This is one of the major criticisms of an evidence based approach. and none of the articles online have covered it well enough. I have read and heard people who are supposed to be experts in scientific approach throw up their hands in despair when they see conflicting studies on the same topic.
So what is wrong with this argument?
Comparing apples & oranges: The most obvious reason is that there are actual differences in the studies though they seemingly appear very similar. The major reasons could be due to the population studied, the intervention/treatment, the outcome measure, the length of the time, and bias. For example, you could have two studies with the same weight training program, muscle mass as the common outcome measure, same length of the training program and still have conflicting results. Why? It is because one study used trained subjects and the other study used untrained. The untrained obviously made a big improvement, while the trained didn’t make much of an improvement as expected.
The point is event though the study may appear similar, it is different in certain fundamental aspects and hence cannot be grouped together in the first place. It is as stupid as saying apples and oranges are conflicting!
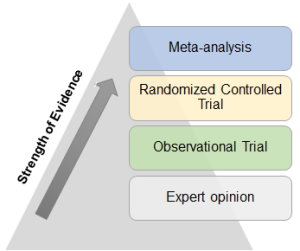 ”
”
Similar Studies Conflict: When similar studies do conflict, it is largely due the reason that studies didn’t have enough subjects. In other words, the treatment is effective, but it wasn’t statistically significant due to a low sample size. We knew this long back and we also have an elegant solution to this problem called meta-analysis. In simple terms, meta-analysis is the systematic process of combining small studies to make one big study with a large number of subjects. In fact, this is the exact reason why meta-analysis has the greatest validity and occupies the top of the pyramid in the hierarchy of evidence in an Evidence based approach.
So people who cherry pick favorable studies to support their statement or who argues that studies are conflicting hence studies are worthless are both wrong and clearly unaware of the basics of an evidence-based approach.
Blah blah,.. can you give an example?
Here is a very famous meta-analysis which looked to see if a short, inexpensive treatment of corticosteroids given to pregnant women will reduce babies dying from the complications of immaturity. The results of this meta-analysis are shown in the figure and is called a forest plot.
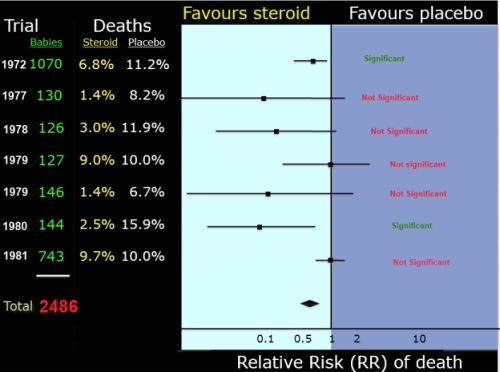
Now what the heck does all those lines mean?
Based on this ‘inconclusive’ evidence, most obstetricians never gave corticosteroids therapy. In 1989, finally, a meta-analysis was conducted. As shown in the figure, when the same, previous studies were combined to get a total of 2486 subjects, there was a very clear benefit of corticosteroid treatment. The position of the diamond to the left favoring the steroid treatment shows that the odds of babies dying prematurely is reduced by 30 to 50 percent with steroid treatment!! Unfortunately, it took another decade and another 10 studies and another meta-analysis for the treatment to be routinely practiced by obstetricians. So we were late to do a meta-analysis, and when one was done, we didn’t bother to look it up and still kept wasting money on new studies. And what does that mean?
That just simply means that tens of thousands of babies probably suffered and probably died needlessly!

In fact, the story was so powerful that they adopted the forest plot of the corticosteroid meta-analysis as the logo for the Cochrane Group. The Cochrane Collaboration is an independent nonprofit organization represented by more than 130 countries. Their primary role is to publish high quality systematic reviews and met analysis in timely manner in the field of health care so that tragedies like these are never ever repeated. If you have questions about healthcare or medicine, this is where you should look first.
The corticosteroid meta-analysis example is an unbelievable story of the power of evidence-based approach, or more specifically the story of meta-analysis, in saving tens of thousands of lives.
Conclusion
Related Articles

Becoming a Supple Leopard by Kelly Starrett: Book Review
August 17 2013
If you are a regular reader of exercise biology, you ought to have read some of my posts about the functional movement screen and about pain treatments. My interest in physical therapy dates back to my early personal training years and to my own struggles with low back pain. Anyway, I have been hearing a lot about Kelly Starrett who seems to have taken the crossfit and strength & conditioning field by storm. So finally checked out his national bestseller book Becoming a Supple Leopard.
Who is Kelly Starrett?
From his blog: Kelly Starrett is a coach, physical therapist, author, speaker, and creator of this blog, which has revolutionized how athletes think about human movement and athletic performance.
What is the book about?
As usual, the book, Becoming a Supple Leopard, starts with an introduction and then goes into the cause of injury and pain. According to Kelly Starret, 100% of all injuries and pain are due to movement dysfunction. Out of this 2% is due to pathology (cancer or something serious) and catastrophic injury, like being hit by a car and so forth. But 98% of the dysfunction is due to missing range of motion and moving in bad position, (like rounded back, and rounded shoulders, feet turned out and such).
So the book is all about fixing those movement dysfunctions and hence preventing/treating pain and injury.
Is this approach revolutionary? The book synopsis (back of the book) says it is a revolutionary approach. And Kelly Starrett writes in the book “Is what I teach radically new? Yes and no.”
I say “No and no”.
These concepts surrounding injury/pain caused by bad or suboptimal posture and movement can be traced back to the 1950’s. Recently, Gray Cook has introduced this line of reasoning into the strength & conditioning field with his FMS. The posture-pain concept has been popularized by Florence Kendall and the movement dysfunctions by Shirley Sahrmann. The majority of people discussing this topic are just regurgitating their work. And what is more important is that these concepts are are based solely on this outdated biomechanical of pain which has now been replaced by the biopsychosocial model of pain.
Three Concepts: He basically outlines his approach in ‘Becoming a Supple Leopard’ to make you move optimally into three basic concepts
Again, nothing new besides the terminologies. Rule 1 means just make sure have a stable core/neutral spine and don’t round/extend your back. All good I think. Then Kelly Starr starts talking about sitting and standing position. Kelly writes”

After reading this part, I honestly didn’t want to read anymore. This was one of the best examples of fear mongering and bad science that I have read. He is literally taking your hand and walking you back to the dark ages of physical therapy of the 1950’s, when we used to believe pain comes from joint, tissues, bad posture and movement. . I wrote an article back in 2005 about the myth of posture and pain and ended the article saying “Now close your eyes, take a deep breath, slowly slump – and savor the freedom of movement”. That time I thought this would be common knowledge in a couple of years. It is 2013 and we are worse off.
And there is no excuse for a PT - or for someone who claims to be at the forefront of treating pain and has a national book seller - to at least make a passing reference to what the current pain science says when you write a 400 page book! At least write, this is the current model (mind you with a lot of evidence), but I get results this way or I don’t agree. Kelly Starrett loves to talk (podcast & videos) and write about the Japanese swordsman who lived 350 years back and who said to make your combat stance your everyday stance. I am like, for heaven’s sake, forget the Japanese fisherman books and please read Patrick Wall, Melzack, Moseley, Louis Gifford who are the pioneers in pain science and who have been talking about the biopysycosocial model of pain since 1970! In this day and age, where you have access to every journal article, blog, podcast readily available in your living room, I am at loss to find an excuse. For me, it is either just intellectual laziness or just being blatently dishonest with your followers.
Anyway, the second rule called the one-joint-rule is pretty much the same as the first rule. Keep your spine braced and movements should be in your shoulders and hip. So if you squat, shoulders and hip should move and the spine should stay put. The third rule is how you should keep your joint tight in their capsule. So screwing your feet on the floor or breaking the bar in bench cues are just helping the mobile joints to stay put in the capsule. I don’t see anything new in these cues besides the fact that they have been organized better.
The next two sections in the book “Becoming a Supple Leopard” are about movement and systems.
Kelly has done a great job when it comes to the design and readability of the book, the pictures are very clear with white backgrounds, plenty of white space, instructions are broken down well, and laid out on a high quality paper and cover material. He is planning to write a new book for the average Joe, which I predict will be based on the same outdated and unscientific concepts of pain, plenty of fear mongering tactics and no single scientific reference to back up any of his claims.
Check the below articles & podcast before commenting please:
Reference
my recent article on pain
Podcast by Jason Silvernail: Here is a podcast which explains everything about the link ( or lack of link) between pain & biomechanics:
Related Articles


Is it Better to be Overweight?
July 06 2013
This is one study that everyone should be aware of, and this is especially true if you work in the fitness or health field. The study is a collection of studies and looked at the association between BMI and deaths (or mortality).What is BMI or Body Mass Index?
BMI or Body Mass Index is commonly used as a measure of your body fat. It is calculated by having your weight divided by height square (kg/m-square). You can calculate your BMI using this calculator. Once you find your BMI, you can see from the chart below if you are normal weight, overweight or obese. And this is true no matter which country you live in. So what is your BMI? 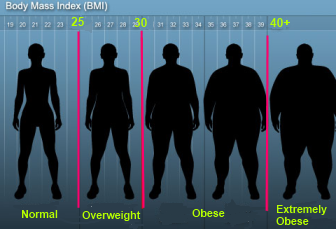
What was the study?
The study published in 2013 in JAMA was done to see how BMI is associated or related to death (or mortality). Or to answer the question who lives the longest? Normal weight, overweight or obese people? What is unique about this study is that that for the first time they looked at more than 7000 studies all over the globe. After this comprehensive analysis, 97 studies were included in the study which looked at more than 2.88 million individuals and 270,000 deaths. This is by far the largest meta-analysis done on this topic.What were the results?
Now here is the fun part: If I plot the BMI ( 18-40) on the x axis and mortality on the y-axis, how would the curve look like? It should be an linear relationship suggesting as BMI goes up, mortality goes up, right? WRONG. As you can see from the graph below,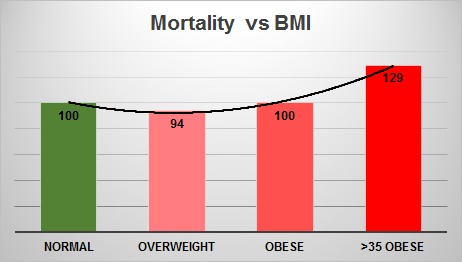
Now what were the criticisms?
As expected, the article garnered a lot of opinion and criticism from both researchers and the press. For me the worst part was none of the experts were specifically responding to the criticisms; they were just beating around the bush.
1.The loudest and harshest of all of them were Dr. Walter Willett, a leading nutrition and epidemiology researcher and the chair of Nutrition department at the Harvard school. He wrote “This study is really a pile of rubbish, and no one should waste their time reading it”. Specifically, he wrote that the study is flawed because the normal weight group contains persons who are lean and active, heavy smokers, frail and elderly, and seriously ill with weight loss due to their disease so there were more deaths in the normal weight.
What could be the explanations?
Now what could explain why being a little fat helps people live longer? Keep in mind that study shows only an association and the decrease in mortality may not have much to do with the extra weight. Here are some of the major reasons quoted (7):
Now what is this 6% decrease in mortality mean?
This study showed a hazard ratio of .96 for the overweight group or a 6% decrease in mortality in the overweight group. But what the heck does this 6% mean to you? This is one important question that almost all articles reporting this study have ignored or missed.
One way to communicate risk is in the form of life-expectancy. For example, a hazard ratio of .96 for a 35 year old means he may add 6 months to his life-expectancy by staying overweight or he may gain 15 min extra everyday. If you are obese (>35), you lose an hour and half everyday. So even if it shows a decrease in mortality with being overweight, it is just very a small effect. This is is the concept of microlives (1 microlife = 30 minutes of your life expectancy) developed by David Spiegelhalter (a very good biostatistician) to communicate health risks to the public (6).
Practical Recommendations
Related Articles


Muscle Memory Solved
March 17 2013
Muscle memory is what? We all know that if you lift weights and stop lifting for a few months (3-6 months), you will lose strength and muscle. However, if you start training back again, you gain the lost muscle or strength within a few weeks - as if the muscle remembers where you left off. This phenomenon is called ‘muscle memory’.

We used to believe this is largely due to the nervous system mechanisms. The nervous system mechanisms may explain the strength gains, but it doesn’t explain how you can gain back the muscle size so quickly.
But recent studies show that we may have finally solved the mystery of muscle memory
How did they solve it?
Unlike other cells, muscle cells have more than one nucleus (probably thousands). So why do muscles need so many nuclei? The nucleus is basically what controls the cell and since your muscles are a lot lot bigger and way more complex than other cells in the body, one or two nuclei just cannot do the job. So when your muscles get bigger, you have to add more muscle nucleus. The increase in nucleus with muscle growth has been shown in number of studies. It has been shown that people who take steroids and people who grow muscle easily have lot more muscle nuclei than normal.
Just like muscle growth, we believed that when we lose muscle, the opposite happens - we lose some nuclei since there is no reason for the extra nuclei to sit around. And this was supported in studies which showed as muscle shrinks in size, the number of nucleus decreases too.
Now here comes the surprise.
However, recently, studies using different animal models (denervation, unloading, synergic ablation) showed that as muscle atrophies or shrinks due to inactivity or detraining (until 3 months), there is no loss of muscle nuclei as we previously thought! As shown in the picture, the muscle size decreased by 50% (lines) but the muscle nuclie count (stained with green dye) remained the same.

So what? Since now the muscle has the same number of muscle nuclei after we stopped training, it is easy to build the muscle back to its previous size. So these muscle nuclei seems to acts like ‘memory cells’. They know how much muscle you had before you stooped training.
But why did we think muscle nuclei die with muscle loss?
The recent studies used a different technique to study these nuclei.
In previous studies they were counting nuclei which belonged to the connective tissue and other cells (satellite cells). And these nuclei do die with detraining. So researchers mistakenly assumed that the muscle nuclei die with muscle loss. But these weren’t actual muscle nuclei. The recent studies only counted the actual muscle nuclei and showed no loss .
Implications
Reference 1
Reference 2
Reference 3
Related Articles





Why should older people do power training?
February 26 2013
One area which you don’t see a lot of articles and discussions among trainers and fitness professionals is the training of older folks. And it seems like this area has become even more important with the all the health insurance crisis we are going through lately.

We know that as you get older strength training becomes critical, but it seems like power training maybe even more important.
But what is power?
Strength is the ability of muscles to produce force, whereas power is the ability of the muscles to produce force more quickly or rapidly. For example, if person A does one rep of bench press at 3 sec, while person B does the same weight in 1 sec, B has greater power.
Why older folks need power than strength?
Muscle loss: Once you hit your 40’s and 50’s, there is a steady decline in muscle mass. This decline in muscle mass (called sarcopenia) could be partly due to reduced activity and decreases in anabolic hormones with ageing.
Also, with ageing you seem to lose one specific type of muscle more than the other. There are two types of muscle fibers: Type 1 and Type 2. Type 2 fibers are the fast fibers or the power fibers. They are the fastest and the strongest and can produce power 2-4 times more than type 1. Unfortunately, with ageing, there is a preferential loss of the number and size of the these type 2 fibers. Guess what happens when you lose the fast or power muscle fibers?
Functioning: In older folks, what is important is physical functioning. It doesn’t matter if you can bench a lot or has a six pack, but can’t do your daily functions. Function is the most important factor affecting quality of life. Below is a nice picture of how loss of strength and power can gradually lead to functional limitation and finally disability. This is when your quality of life goes down, you become dependent on others, gets admitted to nursing care facility and things turn a bit sad from there onwards . So one of the critical questions in ageing research is how can we improve physical function in older people and prevent this slippery slope towards disability.
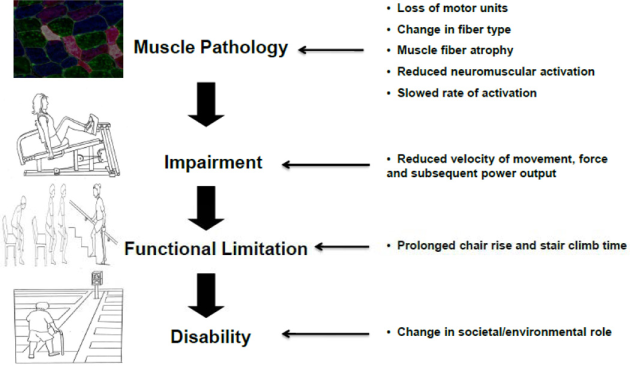
Strength or power? : Number of studies have shown that power to be associated with the ability of older adults to perform activities of daily life such as walking, climbing stairs, rising from a chair and so forth and is considered to be a stronger predictor of function than strength. Power is also a stronger predictor of falls than strength. Also muscle power declines at faster rate than strength (3-4% vs 1-2%)
So the bottom line is power maybe more important than strength in older folks.
So is power training better than regular resistance training?
Not all, but a few studies have shown an increase in power with power training than regular weight training. Strength has shown to increase to similar extent in both groups.
A recent meta-analysis looked at the same question and concluded “power raining is feasible for older folks and has a small advantage over strength training for functional outcomes”
However, there are still more questions about the optimal loading for power, volume for power, which functional outcome measures to use, the long term effects, the feasibility in frail individuals and so forth.
Ok so how the heck do I do power training?
Fast reps: When I say power training , it doesn’t mean using olympic lifts and plyometrics. Here power training means just a simple modification - lifting the load as fast possible - and keeping everything else the same.
Majority of the studies used machines, 2-3 sets for major muscle groups for 2-3 days per week and used an intensity around 70%1RM for 8-10 reps.
What about the safety?
Most studies looked at non-frail individuals so we don’t know how frail individuals can perform power training safely.
Until now, we haven’t seen any more increase in adverse outcomes in studies using power training compared to regular resistance training.
For frail individuals, a lower intensity (40% of RM) might be a better option
Conclusion
Reference 1
Reference 2
Reference 3
Power training using pneumatic machines vs. plate-loaded machines to improve muscle power in older adults.
Related Articles

What the heck is Post Activation Potentiation or PAP?
December 26 2012
PAP stands for post-activation potentiation. And now in English: It is the phenomenon by which muscular performance is enhanced as a result of previous contractions.

For instance, If you were to perform a 5RM back squat and then do an explosive movement, like vertical jump or sprinting you would jump higher/run faster than if you did the vertical jump or sprint without the squat.
PAP mainly enhances explosive/power movements and sub-maximal loads. It doesn’t have a large effect on maximal loads.
How do you activate PAP?
Contraction: PAP is usually elicited by a prior sub-maximal contraction (3-5 RM).
Rest Period: After a rest period of 3-10 minutes, there is an increase in power performance.
Ideal Rest Period: As a result of the conditioning contractions, there is an increase in both fatigue and performance . The rest period allows the fatigue to dissipate so that we can take advantage of the performance aspect. If you rest too long, you will dissipate the performance factor along with the fatigue. If you rest too little, the fatigue effect will negate the performance effect.
What are the mechanisms behind PAP?
Recruitment of Type 2 fibers: There is an increased activation of type 2 fibers. Fast fibers are selectively recruited when you do explosive movements.
Calcium sensitivity: The sensitivity of the muscle to calcium goes up. It is calcium which triggers muscle contraction and controls the amount of force that can be produced.
What factors affect PAP?
Here are the factors that can affect PAP from a recent meta-analysis. In the meta -analysis, they looked at 44 different studies.
Intensity: Moderate Intensity (60-85%) conditioning contractions has a greater effect than heavy intensity contractions. (>85% RM) to activate PAP
Rest Periods: Rest periods after the contractions of 7-10 min has a greater effect than rest periods of 3-7 minutes.
Multiple sets: Multiple sets of prior contractions are better than single sets
Trained vs Untrained: Trained and athletes had a greater effect than untrained. Athletes (more experience) had a much greater effect than trained (less experience) . So PAP generally increases with training experience.
What are the limitations?
Acute effect: PAP only last for a few minutes. So not much benefit for long duration events.
Individual differences: The effects of PAP is heavily dependent on the individual. In most studies, the ideal rest period after the conditioning exercise varied among the subjects. PAP also varies depending on the training experience and the proportion of type of 2 fibers.
Now how high can you jump with PAP?
This is the part which most articles and conversations about PAP somehow seems to miss. How big of a difference can PAP make?
There is usually a 3-5% increase in jump height with PAP. In a recent study, one set of 5RM squat resulted in 1.4cm increase in jump height in varsity level rugby players.
Now how big of a difference is 1.4-2 cm you may ask?
This may not sound much, but in the 2102 London Olympics, 2cm was the difference between a gold and a bronze in the Women’s high jump. Could it have a made a difference if these athletes used PAP?
Reference 1
Reference 2
Study_Flier.pdf
Related Articles
All I care about are results and not evidence or science
October 21 2012
This is the number one argument raised when results are questioned for their lack of evidence or when an evidence-based approach is discussed. And you will see this statement said more than a few times by coaches and trainers as if it makes them a cut above from the rest. Surprisingly, I have had friendly debates with people with Ph’d's and who are so-called ‘evidence-based’.

It is clearly one of the most misunderstood concepts and clearly shows a lack of understanding of the term evidence-based approach and how really research works.
What is so wrong with this statement?
Evolution of evidence-based medicine: Most folks are unaware that evidence-based medicine evolved because we weren’t getting results. It didn’t evolve so that smart doctors can explain “how things work” or the science behind their results. And it is the exact same reason why an evidence-based approach evolved in other fields too. There are hundred’s of drugs and treatments that we still don’t know how it works- but we know from randomized controlled trials that we get results. So we use them. Read this article about Why we need an evidence-based approach?.
For example, the landmark studies done by Doll and Hill in the 60’s showed that smoking is bad for you. Mind you, it was only after these studies we came to realize that smoking is indeed bad for you. It showed that as the number of cigarettes being smoked increased, the incidence of lung cancer went up too. These studies never said anything about the how or the mechanisms involved. The largest RCT in women ever conducted is the Women’s Health Initiative study which showed that hormone replacement therapy (HRT) can be bad. This study was largely responsible for women stopping HRT all over the world. And guess what, we still don’t know what are the mechanisms behind it.
Doctors use an evidence-based approach to help their patients live better/live longer. They don’t use an evidence-based approach because they love to discuss science. Have you heard any doctor saying “all I care about are results” though that’s all they care about. Why is that in our field we trainers and coaches have to say this repeatedly in every facebook post and article?
Basic Science vs applied research: People who think that research or evidence is all about explaining “why” or “how things happen” are just completely unaware of this distinction. National Institute of Health (NIH) has funding allocation for both these studies and there is always a huge debate about which research should get more money.
Evidence based approach mainly looks at applied research or direct studies. Understanding the mechanisms behind a treatment do help us to be more confident about the effectiveness treatment or drug and also helps us to generalize the results to a wider population.
For example, from basic science we know that an increase in load or load progression is primarily causing an increase in muscle growth. Hence we don’t have to repeat a study using load progression for every age group or every ethnic group.
People who look at all those complex physiological and molecular pathways and think that research is all about understanding the ‘why’ are just simply looking at basic science studies or mechanistic studies. They then go on and believe that this is how evidence-based approach works. These basic science studies are only specifically intended to understand the mechanisms and not for application (atleast not in the near future).
Results: This one deserves its very own post. Your results, for that matter, even my results, doesn’t mean a thing. Find me a trainer who doesn’t get results. Forget training, find me a homeopath or a energy healing practioner or palm reader who doesn’t get results. They all genuinely think that they get results or the positive results they see is due to their intervention. No debate or argument in any field has yet to be resolved by counting results on each side.
If you are getting results, it just could mean a lot of other things and doesn’t say anything about you as a trainer or your program: When you say you are getting great result, it could also mean:
My whole point is that it is really hard to say that it is because of your personal training/coaching or your custom program that made the difference. It could be due to a lot of other factors too. This is the exact reason why millions are spent on studies to find the effective treatments and drugs. If the anecdotal results were indeed true, all we have to do is find the doctor who gets the most results and just use his treatment approach, right?. Just to show that exercise and diet indeed helps lower insulin resistance or your chances of getting diabetes, we spent 180 million on one study (Diabetic prevention trial).
I do understand the marketing /personal gratification aspects of sharing results, but trying to debate with your results or bringing up your results every time in an intelligent discussion do not speak so highly of your critical thinking skills.
Conclusions
Random Thoughts
Me: I usually do not like to talk much about my personal life in my site like most other bloggers do. I don’t have much to say. But here we go: I just moved to Miami to start my PhD In Exercise Physiology. Hence the long break in my site updates. If you are somewhere nearby and want to talk a bit about science/exercise, email me.
My Site: Exercise Biology was rated as one of the top 25 fitness sites in 2012. I remember people telling me that it such a competitive field that a fitness site will never get noticed. People told me the same when I moved to US from India to be in the field. I am in this field because I am passionate about the field and I love helping people. If you have those two qualities in large doses, nothing can stop you nor slow you down. Thanks for reading Exercise Biology and supporting an evidence-based approach in your life.
Related Articles
Are Deep Squats Bad for your Knees?
June 19 2012
There are lots of articles online about the safety of deep squats, but I don’t think most convey the truth or the uncertainity involved.

Why deep squats were considered unsafe?
Knee Stability: In 1960, Klein showed that olympic lifters who performed deep squats had an increased incidence of ligament laxity compared to a control group. He also supported his results with a study on cadavers. Based on the in vivo and cadaveric studies, Klein recommended parallel squats than deep squats. His studies led the American Medical Association cautioning against deep squats due to their potential for severe injury.
This led people to believe that deep squats are unsafe.
Why deep squats are considered safe now?
Other Studies: A number of later studies showed that there is no significant knee instability associated with deep squats. Meyers performed a study which had the subjects do deep squats with varying depths. He used the same measurement techniques as Klein and did not find any knee stability issues with deep squats.Chandler did another study comprising of powerlifters, olympic lifters and a control group and concluded that the squat did not have negative effects on knee stability and may be considered safe in terms of not causing permanent stretching of the ligaments. There are other studies to show that there is no excessive movement of the knee that could indicate knee instability due cruciate or collateral ligament damage.
Since the above studies goes against Klein’s conclusion which started the whole ‘deep squats are unsafe’ message, people now believe the exact opposite conlusion- that deep squats are safe.
What is wrong with both the conclusions?
Cartilage and meniscus: The greatest potential for injury with deep squats would be to the menisci and cartilage. But Klein and other studies were looking at knee stability (determined by ligament laxity) instead.
So we were all focusing and basing our conclusions looking at the wrong tissue.
Compressive Forces: Both patellofemoral and tibiofemoral compressive forces are highest at maximum knee flexion. There is usually a small decrease in patellofemoral forces in higher knee flexion angles due to increase in patella contact area. But this only results a slight decrease in force, and this where the confusion arises. So the authors would say there was no significant difference in patellofemoral forces at 70 and 110 degrees. This doesn’t mean that the forces are the same.
For example, in this squatting study there was no significant difference in peak patello femoral stress between the three squatting depths (70, 90 & 110 degrees) (P=.35). But if you look at the forces (10.8, 11.7 and 12.3 Mpa) it is clear that they are increasing with deeper knee angles. So at 135-150 degrees (deep squats), the forces will be at the highest. The forces are increasing and if they used enough sample size, they will find it statistically significant too.
Since the forces are high, there is greater risk of damage to the cartilage and menisci with deep squats. So we cannot conclude that deep squats are safe.
Ideal study: The ideal study to test if deep squats are bad for knees is not an 8 week study or a study which looks at compressive or shears forces as we have seen. What we need is a study where a large group of people who deep squat and another group of people who does parallel squat are followed for 15-20 years. If deep squats are bad for the knees, you will see more people with knee pain in the deep squat group.
The problem with picking a bunch of olympic lifters and testing their knees for damage and pain is that the people who already had knee pain or other problems might have stopped squatting or switched to paralleled squatting. The people who are already deep squatting might be the ones who were blessed with some good knees or have better squatting biomechanics and so forth
Unless we have study like the above, we can never conclude anything about deep squats and safety with certainty. Just like in most cases, we are just simply leaning towards a side based on our personal experiences and observations and just confidently concluding.
Science and anecdotes: Usually in these type of articles, pictures of lifters (look above) doing ass to the ground squats with heavy weights is added just to seal their argument of why deep squats are safe. As I wrote, this doesn’t add anything to a scientific discussion. People who write scientific articles shouldn’t mix their personal experiences or observations or results. That is defeating the whole purpose of using scientific studies. It makes as little sense as one of those swiss balls that comes with a stand for people to sit on. If you are unaware, a bosu ball is used to create an unstable environment. But by using a stand underneath the ball and hence making it stable, you are just defeating the whole purpose of using a bosu ball.
Practical Applications
Reference 1
Reference 2
Reference 3
Related Articles


Does Foam Rolling Work?
May 27 2012
Foam rolling is a form of self massage which involves rolling your body parts on a cylindrical piece of foam.

Claims: It is claimed that foam rolling will help improve range of motion, decrease soreness, and relieve pain. As expected, lot of athletes use it though there is not any evidence to back it up. Some do it before the workout and some do it post workout.
Recently a study was published which looked at foam rolling and its benefits. Let’s take a closer look:
What was the foam rolling study design?
My Comments
Just reading the conclusion of the study will make you believe that foam rolling helps and you should start foam rolling. But that is clearly not how an evidence-based approach works. Before you read this, I would take a look at Greg Lehman’s critique of the study in his blog (Body Mechanic). He wrote a lot of great comments which I have listed below too. I have added a few more below.
Randomization: This was a within-subject design. That is, one leg acted as the experimental group and the other leg was the control. But they just simply used the right leg for the foam rolling and left leg as control. The leg that received the treatment should be randomized. And this is not a minor criticism. Randomization is overlooked by many people, but is one of the most critical components of an RCT. Hence the name ‘Randomized’ controlled trial.
Control Group: There are two problems with the control group:
Flexibility Measurement: The knee ROM was measured with a goniometer.

Acute Design: The study design is acute. We don’t know if these flexibility or strength measurement will stay the same if the study was carried out for 6-8 weeks.
What about the application of foam rolling?
What about coaches and athletes getting results with foam rolling?
Results: I have repeated this again and again: The term ‘results’ is just too vague to make any meaningful conclusions. Results may be (and this is a big maybe) true, but the question is can it be attributed to that one variable out of hundreds of variables. It is funny when coaches claim foam rolling is good because they are getting results and hundreds of athletes are using it. Now here we go about results:
And as a side not, here is what Mike Boyle - a leading strength coach - has to say in his blog about why he uses foam rolling in reply to Greg’s post (and why others should use it). I am still trying to figure out what he meant.
So, back to why we foam roll. In the simplest sense, rolling is step one on the preparatory process. Our goal pre-exercise is to prepare the tissue for the stresses about to be applied. Proper tissue preparation allows an athlete to perform a workout without injury. I think or hope that we can accept the position that tissue changes in response to stress.If the tissue is stressed optimally, the resulting adaptation is positive. If the tissue is overstressed by inappropriate volume (too many reps) , speed of lengthening (too fast) , or inappropriate overload (to much weight) the tissue response can shift from positive to negative. Although tissue soreness is deemed normal, we must acknowledge that there is an ideal amount of that normal response, and the response should be limited to the muscle tissue and not be present in the connective tissue. In other words, sore quads would be OK, but sore knees not be OK.
NOTE: The article is about the analysis of the foam rolling study which looked at foam rolling as a warm up. I haven’t talked about the use of foam rolling for pain or relieving soreness.
Reference
Reference 2
Reference 3
Related Articles
How to be Happy in Life: A Scientific Approach
May 15 2012
We do everything in our life with one single goal: to be happy. Everything in our life we do can be narrowed down to this one goal.
Pick a Men’s Health or Cosmo magazine or talk to your friend and you will get plenty of tips and recommendations to be happy. But the question is do they have any scientific evidence? I would say very little.
Sonja Lyubomirsky is one of the leading researchers in the field of happiness. She has been doing research on happiness for more than 20 years. In this article, I will be writing some of the key points made in her book: The How of Happines. You will also find a short interview with Dr.Sonja Lyubomirsky at the end of the article.
If you like to be happy, this will probably be the most useful article you will ever read.
Can we be more happy in life?
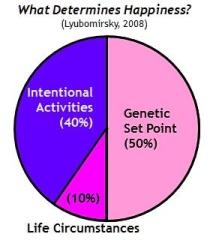
Happiness Pie: A decade ago most researchers thought that people couldn’t increase their happiness permanently. Now studies show that 50% of difference in people’s happiness can be accounted by your genes. The most interesting finding is that only 10% of the variance is explained by your circumstances (rich or poor, unhealthy or healthy, married or divorced and such). The remaining 40% of the variances lies in our behavior or our intentional activities!
Can material wealth or being beautiful make us more happy?
Though this is hard to believe, whether you drive to work in a lexus or a battered truck, whether you are young or old, or have had wrinkle-removing plastic surgery, your chances of being happy or becoming happier are much the same.
US Study: In 1940 in United States, one third of homes didn’t have running water, indoor toilets, or bathtub/showers and more than half had no central heating, When asked to rate their overall happiness,, they reported being very happy with an average score of 7.5 out of 10. The typical household today has running water, two or more baths, central heating, not to mention microwave color TVs, DEV players , I-pods’s and computer. Now guess what our average score is? 7.2! That is, all that new gadgets and material wealth could not make us more happier.
Once you have the basic needs of life fulfilled, it seems like that relationship between money and happiness decreases. The richest Americans, those earning more than 10 million dollars annually, report levels of personal happiness only slightly greater than the office staffs and blue-collar workers they employ. We have now a lot of evidence to show that spending money on things which help us grow as a person (taking guitar lessons, learning a new skill) or new experiences (going scuba diving, family reunion) or spending on small things than just one big item ( like a new car of big flat screen) tend to make us more happier than buying material goods.
Beauty: The number of plastic surgeries to make people look good has gone up to millions. Most people report being satisfied with post surgery physical appearances - but only for a short period of time. Research has shown that good looking people aren’t any more happier. In fact, there is evidence to show that happier people tend to perceive everything about their lives to be more positive and optimistic.
Why do life changes account for so little happiness? The answer is hedonic adaptation: We tend to adapt or our senses tend to adapt to these changes pretty quickly - that is, we get used to relocations, marriage, job changes, a new car and so forth.
How to be more happy in life?
These are the 12 scientific recommendations in the book that you can take advantage of. The book goes much more in-depth and reference a lot of studies.
Practicing Gratitude & Positive thinking| Express gratitude: Or count you blessing. Keep a gratitude journal and jot down 3-5 things which you are thankful for once a week.
It could be just the wonderful coffee you had the other day or just unforgettable moments like graduating college or having a baby. Keep it fresh by how you express your gratitude. You can talk to a friend instead of writing it down in your journal. You can express gratitude directly to the person - by phone, letter or face to face.
Cultivating Optimism: Basically means looking at the brighter side of things in life. Some of the ways shown in research is the ‘best possible selves’ diary
Sit in a quiet place and take twenty to thirty minutes to think about what you expect your life to be one, five or ten years down the road. Imagine a future where everything has turned out to be how you exactly wanted. Identify barrier thoughts - Write down your barrier or negative thoughts and ask yourself questions like, what else could the experience earn? Can anything good from it? What lessons can I learn and apply in the future?
Avoid Overthinking: Number of studies has shown that ruminating or over-thinking over problems can make worsen sadness, fosters negative thinking, saps motivation and so forth.
Distract yourself by watching a funny move or going to tea with you friend. A second technique is to stop technique where you think or say stop when you start over-thinking or making comparisons. Another strategy is writing down you negative thoughts.
Invest in Social Connections | Practicing Act of Kindness: What research has shown is that practicing kindness is not only good for the recipient but also for the doer. It could be a small deed such as a sincere smile and thank you to a passerby.
The important thing is here to keep varying the act of kindness you do. If you do the same thing, you will adapt it to it pretty soon. Like most of the recommendations, it takes some effort and creativity to vary things up. For example, if you are short of money, give the gift of time - Offer to make a repaid, weed a garden and so on.
Nurturing Social Relationships: One of the biggest factors in happiness appears to be maintaining strong personal relationships. This strategy involves putting effort into healing, cultivating, and enjoying your relationships with family and friends
Some strategies include making time for an important person in your life (could be your wife or friend), express admiration and appreciation, be supportive and loyal when your friends needs it and enjoy their success.
Managing Stress Hardships And trauma | Learn to Cope: Coping is what people do to alleviate the hurt and stress caused by a negative event in life.
There are lots of studies showing benefit to expressive writing. The procedure involves writing about your most traumatic experience of you entire life. You just go and explore your deepest emotions and thoughts, You should write about 15 minutes writing each day for several days in a row.
Learn to forgive: This is one area where there is plenty of research and anecdotal evidence exists. Let go of anger, resentment, and feelings of vengeance by writing – but, not sending – a letter of forgiveness to a person who has hurt or wronged you. In this exercise called expressive writing identify the person who you blame for mistreating you offending you.
Another way is to practice empathy: Empathy involves understanding other person’s thoughts and emotions. One way to practice empathy is to notice every time someone who does something that you don’t understand. Try to work out their feelings, limitations or why did they do it or what factors might explain it.
Living in the Present | Increasing Flow Experience: When you’re so absorbed in what you’re doing that you don’t notice the passage of time, you are in a state called “flow,”
So, become fully engaged at work, at home, and at play. Try to increase the number of flow experiences in your life, whether it’s completing a project at the office, playing with your children, or enjoying a hobby. Seek work and leisure activities that engage your skills and expertise.
Savoring Life’s Joy: Pay close attention and take delight in momentary pleasures, wonders, and magical moments. Focus on the sweetness of a ripe mango, the aroma of a bakery, or the warmth of the sun when you step out from the shade
Committing to your Goals: People who strive for something significant, whether it’s learning a new craft or raising moral children, are far happier than those who don’t have strong dreams or aspirations. Find a happy person and you will find a project. That being said, being dedicated to any pursuit won’t make you happy if you’re just doing it for superficial reasons such as making money, boosting your ego, or succumbing to peer pressure.
Pursue intrinsic goals than extrinsic goals for superficial reasons like making money, boosting your ego or seeking power or fame. Perceiving intrinsic goals are more likely to make us happy because they are inspiring and enjoyable, hence we are more likely to persevere and succeed at them.
Taking Care of your body and Soul:Getting plenty of sleep, exercising, stretching, meditating, smiling and laughing can all enhance your mood in the short term and promote energy and strong mental health. Practiced regularly, they can help make your daily life more satisfying and increase long-term happiness.
Should I do all of them?
Best Fit: It is emphasized in the book that you pick the ones which you think will enjoy the most and hence will stick to it the longest. So you don’t have to do all of them. And yes it takes effort to and commitment to be happy.
I asked a couple of questions to Dr.Sonja Lyubomirsky and she was kind enough to answer them.
1. Which strategy has the most support in research. I know it depends on the type of the person and circumstances. But which has the most number of studies and which shows the greatest magnitude of effect?
Hard to answer but most likely gratitude and in particular writing gratitude letters.
2. I see that most studies are weeks or months in duration. Do you think long terms studies lasting years have been conducted and show the same results?
Excellent point- We always say, just like with a prescription, you have to keep taking it for it to continue “working.” The longest follow-ups are about 9 months I think (where the effects are still observable.)
3) Any new books you are planning to write?
Yes, already done. I have a book coming out in January 2013— see below:
Lyubomirsky, S. (in press). The myth of happiness: What should make you happy, but doesn’t, what shouldn’t make you happy, but does, what happiness really is – and isn’t. New York: Penguin Press.
4) Any other book recommendations?
My favorite recent (nonfiction social science-type) books have been Gilbert Welch’s Overdiagnosed and Bryan Caplan’s Selfish Reasons to Have More Kids.
Now have a smile and express gratitude by sharing this post on Facebook or emailing it your friends please. As always, Exercise Biology will give you the most unbiased scientific information you will ever find to keep you healthy and fit.
Related Articles
Growth Hormone Supplements Work for Bodybuilding?
May 04 2012
Do growth hormone supplements increase muscle or help in bodybuilding? A lot of athletes and body builders have been caught using growth hormone. But does it really work? If it works, are there any side effects?
What is growth hormone?
Growth Hormone: Growth hormone is a hormone which is required for growth, especially during adolescence.
Age Effects: As you get older the GH levels get lower. A 60 year old male will only produce half the level produced by a 20 year old in a day.
Do growth hormone supplements really increase muscle?
What are some of the growth hormone effects on muscle and strength?
GH Deficient Children: GH has some clear beneficial effects in children who are growth hormone deficient.
Muscle Wasting Conditions: In 1990’s, Growth hormone was considered the magic pill to manage muscle loss in these diseases such as aids, sepsis and so forth But the evidence of building muscle or maintain muscle is just lacking.
GH Deficient Adults: In GH deficient adults, there is a decrease in strength and muscle. But studies (less than a year) have shown there was no increase in strength or muscle with GH supplementation. Long term studies, over 1- years have shown small increase in strength.
Healthy Adults: In healthy adults, GH shows an increase in LBM:
The bottom line is growth hormone doesn’t work for bodybuilding, especially if you are a healthy adult.
Why bodybuilders use growth hormone supplement?
Tradition: GH has long been thought as an anabolic hormone. And most people are unaware of the recent scientific studies.
Other Hormones: GH is just one supplement out of tens of supplements bodybuilders take. So they got no clue if their increase muscle is due to growth hormone or testosterone. They just think it helps. And there is a beneficial effect when GH and testosterone is combined.
Body fat: GH has some beneficial effects on body fat and hence may be useful for bodybuilders.
What are the side affects of growth hormone supplements?
GH may not have many beneficial effects for bodybuilders, but Growth hormone side effect are plenty.
Acute Side Effects: Growth hormone side effect in healthy adults include, pins and needles, carpal tunnel syndrome and arthralgias. Other growth hormone side affects including sweating, fatigue and dizziness.
Long term side effects: The side effect of growth hormone in the long run include diabetes and heart problems
Acromegaly: Acromegaly is a condition where the body releases excess growth hormone. People with acormegaly usually increased rates of cardiovascular disease, diabetes, osteoarthritis, and breast and colorectal cancer. Bodybuilders who take GH for long period of time could have similar side effects as those people with acromegaly.
Practical applications
Related Articles




Does Testosterone Supplement Tribulus work?
April 23 2012
Testosterone supplement tribulus is sold as a supplement for bodybuilding. But does it work for building muscle and strength?
What is this testosterone supplement tribulus?
Tribulus Terrestris is a herbal supplement often used in folk medicine to improve sexual performance and physical performance in men (aphrodisiac).
What are the claims made by tirbulus supplements?
Increase in testosterone: It is claimed that tribulus will significantly increase testosterone or testosterone precursor levels.
Increase in Muscle and Strength: This increase in testosterone will show up as an increase in muscle mass and strength in people who are weight training.
Are there any studies done on Tribulus?
There are a few studies which looked at Tribulus as a testosterone supplement
Tribulus study 1: This study was done on elite level rugby players randomly assigned to a tribulus and a control group. They took 450mg/day of tribulus terrestris for 5 weeks and performed weight training. After 5 weeks, there was no statistically significant increase in muscle mass or strength.
Tribulus Study 2: This study was done on healthy young males. They took 10-20mg/kg of bodyweight daily for 4 weeks. The study showed no significant increase in testosterone levels.
Tribulus Study 3: This study was done on 15 young males randomly assigned to a tribulus and a placebo group. They took 3.21mg 6-8 tomes daily for 8 weeks and performed weight training. The study concluded that there was no change in body composition or exercise performance with tribulus supplementation.
Tribulus study in Animals: There are a lot of studies done on rabbits and rats which showed increase in testosterone and other androgen hormones. Too bad that I don’t have any rats and rabbits as subscribers.
Are there any side effects of Tribulus?
No side effects have been reported in studies. This would have been great news if it had some good effects too.
Practical Application
Reference 1
Reference 2
Reference 3
Related Articles


Jeff Rodriguez - The Frank Zane of Natural Bodybuilding
April 17 2012
Jeff Rodriguez is a natural bodybuilder, and is one of the best natural bodybuilders out there. As you can see his conditioning, muscle separation and symmetry is just of the world. Jeff Rodriguez is indeed the Frank Zane of natural bodybuilding.

Jeff Rodriguez competes in the NPC (National Physique Committee) competitions. He recently won the overall at the 2012 NPC California Governor’s Cup. To compete in the Mr. Olympia, Arnold classic and other pro bodybuilding shows, you have to win the overall (or sometimes your class) at a national level, professional qualifying NPC show. Hence most of the bodybuilders in NPC are using some special ‘vitamins’. You have to have some amazing genetics to be a natural bodybuilder and still compete in the NPC. So to be a natural bodybuilder and win is something special. A few of the other natural bodybuilders in NPC who are doing very well are Kiyoshi Moody, Phillip Ricardo, and Dave Goodin.
I have been following Jeff Rodriguez for a couple of years. What I really like about Jeff is that he seems to be very reasonable and rational in his approach to bodybuilding. Jeff is always quick to say that he doesn’t have any special or magic program and his bodybuilding results could be partly due to his genetics too. There are many uncertainties in bodybuilding and Jeff Rodriguez is honest about his opinion on these, and does not shy away from conveying these uncertainties.Here is Jeff Rodriguez for you:
1. Tell us a bit about yourself Jeff Rodriguez (weight, height, occupation, location)?
Height: 5’9” offseason weight: 215, contest weight: somewhere in the 180s. Occupation: Personal Trainer. Location: San Francisco Bay Area, California
2. Since we might get a few questions on this topic, let me ask straight away: I had a lot of comments about this issue when I posted the article “The Top Natural Bodybuilders”. Do you think it is possible to get a physique like yours without steroids?
I’ve done it so of course I think its possible. I think most people do not get close to their natural potential because they either aren’t consistent enough over a very long period of time.
2. What do you think are your favorite body parts, Jeff?
To train? Back, legs, or chest, though I also like training arms. Favorite body parts… I would say it is the general balance/flow/symmetry of my physique more so than any one body part, though if I had to guess what I think people would say, it would be triceps

3. What is your bodybuilding training program like? For example, the frequency, the number of sets and repetition range.
Here is what I am currently doing. I don’t have a specific day I do these on as they fall on different days each week, but I am currently following this order for 2 days on 1 day off. I also do not do the exact same exercises each week, but I will list a typical workout for each day.
Day 1: Chest, Shoulders, Triceps
3x Flat Dumbbell Presses, 4-10 reps
2-3x Incline Plate Loaded Presses (EG Hammer Strength), 6-10 reps
2-3x Cable Flys, 8-12 reps
4x Side Raises (cable, machine, or dumbbells), 6-12 reps
3x Lying Triceps Extensions, 5-10 reps
2x Cable Push Downs, 6-10 reps
Day 2: Quads, Calves
3x Squats, 4-10 reps
3x Leg Press, 6-10 reps
2x Something 1-legged (lunges, 1 legged leg press, etc.) 8-12 reps
2x Abductor Machine, 8-14 reps
2x Adductor Machine, 8-14 reps
3-4x Any calf machine, 8-14 reps
Day 3: Back, Biceps
3x Barbell Rows, 6-10 reps
2-3x Plate Loaded Pull Down, 6-10 reps
2-3x Dumbbell Rows, 8-10 reps
0-2x Pull Overs, 8-10 reps
2x Barbell Shrugs, 8-12 reps
3x Dumbbell Curls, 6-10 reps
3x Cable Curls, 6-10 reps
Day 4: Hamstrings, Abs, Calves, Rotator Cuffs
3x Lying Leg Curls, 6-10 reps
2-3x 1-Legged Leg Curls, 6-10 reps
0-2x Seated Leg Curls, 8-12 reps
3x Crunches (cable or dumbbells), 8-14 reps
2x Reverse Crunches (hanging or lying on bench), 8-14 reps
4x Any Calf Machine, 8-14 reps
3-4x Rotator Cuff Exercise (Dumbbell or Cable) 10-16 reps
4. What do you think of failure training? How often do you go to failure? Do you do forced reps, drops sets and other bodybuilding intensity techniques?
I do not train to failure every set. I usually stop a bit short of true failure and only complete reps I can complete on my own. For example, if I had 8.5 reps on a certain exercise, I would perform 8 reps, then stop. No, I do not do any of those techniques.
5. For people who want to put muscle, what are the 2- 3 most important things in bodybuilding that they should focus on?
That is, its precisely what people should focus on that they neglect in an effort to put on muscle. My top three that people should focus on, but do not, are: 1) nutrition 2) consistency 3) training intensity
My top three that people should focus on, but do not, are: 1) nutrition 2) consistency 3) training intensity
6.Can you write a sample program with exercises, sets (warm up and work), and reps for someone who want to improve his lagging triceps. Imagine his diet is good and he is hitting a muscle group once a week.
I don’t think there is anything special or new I can say here and I think my response holds true for any body part. Let us assume a few things: 1) you’re training them properly, 2) you’re giving them enough rest, 3) your nutrition is allowing you to maximize your goals. With that in mind I don’t think there is really much you can do. I suppose you could try training more, but other than that if you’re doing everything correctly then you’re already maximizing your potential.

However, if one of the above three things I listed are not true, then that’s what you should address. 1) Try training them differently if what you are doing is not working well. 2) make sure you allow adequate rest since you can only beat up a muscle so much, it has to have time to heal. 3) Improve your daily nutritional habits and string together not just a good week or month, but a good year and see where that takes you.
Finally, regarding triceps, here are some specific exercises I like: dips, lying triceps extensions, close grip bench press on the smith machine, push downs using the w-bar/cambered bar.
7. What supplements do you take Jeff?
Whey protein, creatine, beta alanine, dextrose, caffeine, multi vitamins
8. Who are your favorite natural bodybuilders, Jeff?
Just to name a few: Kiyoshi Moody, Tim Martin, and Donovan Strong (I used to Donovan at the Team Universe every year and really liked his physique).
9. What are your future goals, Jeff?
My goal is to win the overall at the NPC Team Universe.
You can follow Jeff on his website or on his facebook page:Website: jrodfitness.com Facebook: facebook.com/jrod.bodybuilding. thank Jeff Rodriguez for taking the time to answer the questions.
Related Articles


Prevent Cancer in 8 Simple Steps
April 07 2012
How do you prevent cancer or can cancer be prevented? My Mom passed away a couple of years back from cancer. So I know how dreadful this diease can be - not just to the patient but also to people near to them. Here are the latest scientific recommendations to prevent cancer. I wish everyone would take the time to read it and prevent cancer
Can cancer be prevented?
Environment: It is more and more clear that only a small number of cancers are inherited. Environmental factors or lifestyle choices seem to have the biggest influence on cancer prevention.
These environmental factors include smoking and other use of tobacco; infectious agents; radiation; industrial pollution; medication, food, nutrition, physical activity, and body composition.
What are these cancer prevention recommendations based on?
These cancer prevention recommendations are based on the second report titled “Food, Nutrition, Physical Activity and the Prevention of Cancer: a Global Perspective” published by the World Cancer Research Fund together with the American Institute for Cancer Research in 2007. This is the most current and comprehensive analysis of the literature on diet, physical activity and cancer prevention.
The report is based on the in-depth analysis of over 7,000 scientific studies published on cancer prevention over the last 50 years
A panel of 21 world-renowned scientists reviewed the cancer research evidence and drew conclusions that led to our current cancer preventon recommendations.
What are these cancer prevention recommendations?
1. Body Fatness: Be as lean as possible within the normal range of body weight to prevent cancer
2. Physical Activity: Be physically active as part of everyday life
3. Foods And Drinks That Promote Weight Gain: Limit consumption of energy-dense foods and avoid sugary drinks to prevent cancer
4. Plant Foods: Eat mostly foods of plant origin to prevent cancer
5. Animal foods: Limit intake of red meat and avoid processed meat
6. Alcoholic Drinks: Limit alcoholic drinks. If alcoholic drinks are consumed, limit consumption to no more than two drinks a day for men and one drink a day for women
7. Preservation, Processing, Preparation: Limit consumption of salt and avoid mouldy cereals (grains) or pulses (legumes) to prevent cancer
8. Dietary Supplements: Aim to meet nutritional needs through diet alone. Dietary supplements are not recommended for cancer prevention. Anybody here taking any supplements which claims to prevent cancer?
Two Special cancer prevention recommendations
Breastfeeding: Mothers to breastfeed; children to be breastfed
Cancer Survivors: Follow the recommendations for cancer prevention
As always, Exercise Biology will only give you the top, unbiased scientific information to keep you healthy and fit.
Please share it with your friends and family.
Related Articles


A New Equation to Calculate the Calories Required to Lose Weight
March 26 2012
How do you use an equation to calculate the calories required to lose weight? It is always said that you need to burn 3500 calories to burn one found of fat. Hence the usual logic is to cut 500 calories per day and you will be losing 1 lb a week. This is called the 3500 calorie per pound rule.

But this never happens in reality.
Why is the 3500C reduction to lose 1lb rule wrong?
Assumption: This calculation is based on the assumption that you are losing 87% of fat. But when people lose weight, they lose muscle mass too.
Metabolic Slow Down: As you lose weight, you also lose some muscle. This loss in muscle causes a decrease in resting metabolic rate.
Calories burned: As you lose weight, your body burns less calories to do the same amount of activity.
Starting Composition: It is now known that people with greater initial body fat levels lose less muscle compared to people with lower initial body fat levels.
How is the new equation different from the old equation?
Old equation: For a 224lb guy, a 500 calorie deficit/week will result in 50lb weight loss in the first year.
New equation: Based on the new model, for a 224lb guy, the body weight will plateau after losing 56 lbs in 10 years. Out of the 56 lbs, you will lose 22lb in the first year and the 95% of the this 56lb in 3 years.
The old equation predicts greater than 100% weight loss than the new equation!
What is this new dynamic equation?
These complex equations to calculate the calories required to lose weight have been integrated into a web-based program.
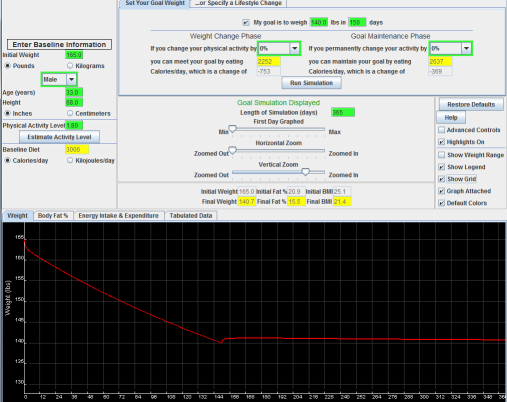
For example, I am 165lb and 68in tall. In the top-middle panel, I have my goal weight (140lb) and desired time interval to achieve the goal (150 days).Running the simulation shows the required changes of calorie intake to meet the goal and then maintain the weight change. The simulated bodyweight trajectory is graphically displayed in the lower panel. Users can also modify the physical activity tosee how combinations of diet and exercise can achieve the same goal.
Click the lick to open the body weight simulator: The New Equation
Limitations
Practical Application
Related Articles




Should you eat protein every 2-3 hours for muscle growth?
March 15 2012
It is said that you should eat protein every 2-3 hours because protein synthesis only last 2-3 hours and your body can only absorb so much protein. So it is typical to see bodybuilders and serious athletes drink or eat protein or amino acids every 2-3 hours.

But can eating protein every 2-3 hours maintain protein or increase synthesis?
Why should you eat protein?
Protein synthesis: A regular meal increases protein synthesis or the synthesis of new protein. Later it was found that this increase in protein synthesis is due to the protein in the food. So eating sufficient protein is important to prevent muscle loss and to increase muscle.
Amino Acids: Amino acids are the building blocks of protein. Just like carbs are broken down to glucose, protein is broken down to amino acids so that it can be used by the body. So availability of protein is measured by the AA levels in the blood.
How much protein: It has been shown that 20 gms of protein or 10 gms of EAA or 3.2 gms of lecuine is enough to maximize or saturate protein synthesis for an average person. Any further protein gets oxidized or burned.
How long does this protein synthesis last?
Few Hours: Muscle protein synthesis should decrease or protein degradation should increase after a few hours (2-3 hours) of eating protein. This makes sense because if protein synthesis increased indefinitely, we all will keep growing.
How long is few hours: To study exactly how long protein synthesis last, they infused amino acids into the blood for 6 hours.
What did the found? They found muscle protein synthesis peak at 2 hours and then returned to basal levels after 2-3 hours. But, strangely, the amino acid levels in the blood were still high!
What about an oral dose of protein?
The infusion study is only applicable to patients who gets protein infusion.
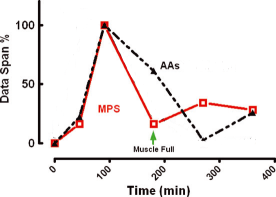
Oral Dose: Instead of infusion, the researchers had young subjects eat 40 gms of whey protein (20 gms of Essential Amino Aacids). And what did they found? As seen with infusion, there was a large increase in protein synthesis which peaked at 1.5 hours, before returning to baseline levels at 2-3 hours. But the amino acids levels in the blood were still high (130% at 2 hours and 80% at 3 hours).
The researchers coined the phenomenon as the “muscle full” effect.
How can we overcome this suppression of protein synthesis?
Spacing Proteins Further than 2- 3 hours: Maybe amino acid levels have to come down to baseline level or below baseline level to re-sensitize muscle and thereby increase protein synthesis. So it maybe better to have protein every 4-6 hours than every 2-3 hours as usually seen.
Practical Applications
Related Articles



Why We Need an Evidence-Based Approach in the Fitness Field
February 13 2012
The article is posted in Brad Schoenfeld's website. Brad is a good friend of mine and is someone who I look upto in the fitness field. Brad is one of the very few who is equally adept at both research and application in the fitness feld.
The article is not for just the fitness enthiusaist but for anyone who is concerned for their health. Without further ado, here you go: Why We Need an Evidence-Based Approach in the Fitness Field
If you ever come across an argument against someone questioning the benefit of science or an evidence-based approach, please use this article. This article is probably the most important article I ever wrote.
Related Articles


The Cause of Obesity - Part 3
January 29 2012
This is the last post on this topic (Part 1 & Part 2). Lot of people made comments and there were a lot of discussions on a few different blogs and forums. I had a posted in a couple of other forums too. I knew very well that I will get a lot of criticisms, but I am sure these articles will will make a lot of people think twice before they make comments about obesity and obese people.
This a very important topic and I admire all those passionate commenters who took the time to express their concerns and opinions. In this article, I will be replying to some of the commonly asked questions about the articles
1. This is just a matter of how you view it. Environment is required for obesity. Look at the concentration camps and tell me how many people are obese, Anoop?
This is one question that was raised lot. This is almost a knee-jerk response from people. It is true that environment is required. I don't think anyone will argue against it. The concentration camp is just an example of the “absence” of environment or the “lack” of environment. If we don't give food, nobody will be obese, or for that matter, nobody will be even healthy or normal weight!
What we are concerned is when everyone is given free access to food (or the same environment) why only a few people become obese? Here is an example I gave to one of the posters. I usually don't try to make analogies because they are often wrong, but I feel this gets the point across.
Imagine you plant Sequoia tree (one of the tallest trees) and other trees in a plot which has the same type of soil (same environment). After a few years, you see the sequoia tree taller than others. Are you going to say the difference in tallness of the trees is because of the soil (environment) or simply because it is the sequoia tree (genetics)? Almost 99% percent of people would simply say it is the sequoia tree. We are not going to sit and argue if it weren't for the soil the tree wouldn't be this tall. But when it comes to obesity, we just can't see the obvious.
2. Just like other genetics disorders, obesity will not manifest if there is no environment.
“Every genetic disorder is 100% genes and 100% environment”, by Ken Rothman (one of the epidemiological greats). A classic example quoted is the phenylketonuria (PKU), a genetic disorder which characterized by a mutation in the gene for enzyme rendering it nonfunctional; this is about as 100% genetic as a disease can get! If it goes untreated, the kids develop mental retardation and brain damage. Nevertheless if there was no phenylalanine given - a phenylalanine free-diet, there would be no PKU, so one could argue it is 100% environmentally determined.
The huge mistake in comparing PKU (or other genetics diseases) and obesity is that in PhenylKetone Urea (PKU) kids are not “hungry” for phenylalanine.
In obesity, hunger is THE fundamental problem. We used to believe that people became fat because they had a slow metabolism or they spent less energy (Non-exercise activity thermogenisis). Now we clearly know that Leptin, Ghrelin and all other staggering complex of hormones are working at the hypothalamus by increasing or decreasing appetite. When leptin deficient kids who have a voracious appetite are treated with leptin, the first thing to drop is their hunger. Kids with Prader-willi syndrome eat from garbage cans because they feel they will die if they don't eat. Bariatric surgery works so well because it is bunting their appetite for some weird reason. People who lose a lot of weight gain weight back because they are primarily hungry.
So obesity is not a “passive” genetic problem where the genes are just sitting there in the background silently until they see food. People eat because they are hungry.
3. Obesity is all about people eating more. If obese people eat less and move more, they will not be obese.
Obese people are fat because they eat too much. Everyone knows that. The question is why are these people doing it in the first place? Or why are 70% of the non-obese not doing the same? Is it lack of will power or laziness when both have access to the SAME toxic environment?
If it is not biology then it should be lack of will power or laziness. If that's the case, we have a bigger issue here. Obese people are lazy and are incapable of changing habits and behaviors. This is so earth shattering discovery that is worth the Nobel Prize in the field of psychology.
4. Ok. Obesity is largely genetics. But there are a lot of people who lose weight and keep it off, right
And this is the problem with anecdotal evidence: looking at a few positives and casually extrapolating to everyone. Nobody wants to write about their tales of weight loss failure or struggles. People only hear (or want to hear) the grandiose tales of weight loss success in magaziines and on TV. And this is just a minority.
The negative hits never get counted or talked about. In medicine they say, “dead men never tell any tales”. In research, they count the negative hits too. There are people who are struggling very hard, but still cannot lose weight and keep it off.
Here is one commenter: How interesting! I have struggled with weight all my life. I have gone from a size 16/18 to a size 10/12 without ever going below 65kilos. It is as if my body simply will not release any more weight. Also, I recently lost 5kilos over 4 months or so, without losing any fat percentage whatsoever! Again, it just will not go! At size 10/12 I am still 35% fat, and have only ever been 40% fat at my heaviest at 85 kilos. It feels mad!
Her story will never come on a magazine or a blog. She might very well have a biology which makes it hard to lose weight and keep it off. But they are all lumped into the same category and just crucified for not working hard enough or making bad choices. This is an example of how research or science helping morality. We are the very same people who back in the days labeled schizophrenics as possessed by demons and people with complex regional pain syndrome as mad! And what helped them? Science or understanding the biology - not more or better anecdotes.
5. Twin studies show heritability of obesity to be around 60-80% (very high). So 60% of your weight is explained by genes and the rest is environment.
No. Heritability can only explain the variation between individuals within an environment. So when they say heritability of height is 90%, it means 90% of the difference between average height and extremes of height can be explained by genes. We cannot say that this percentage of the weight is due to genes or environment.
6. Everyone can get obese if they eat enough food or have access to enough calories. Look around, people now are fatter than they were in the 70's. How do you explain that?
And this is the number one reason why people instinctively question these articles.
And this is another problem with anecdotal evidence. When people say people are getting fat, they have no accurate way of quantifying the gain in weight. They are just eyeballing and making conclusions. Did they gain 10, 20, 50, and 150? Most people are talking about their 5 to 15 lbs weight they gained or saw their friend gain and extrapolating it to the effect of environment on obesity.
There is no question that people gain 10-15 lbs due to environment. You won't call that fat do you? To go from overweight category to Obese (25 BMI to 30 BMI),you have to gain around 35-40lbs. To go from normal weight to obese (20 -30 BMI), you have to gain around 75-80lbs. To go from normal weight to extremely obese (20-35), you have to gain 125lbs. But if you are right below 30, you can gain just 2-3 lbs and be clinically obese!
Do you seriously think people gain this 50-100lbs weight by “accident” if they have food around?
And it is extremely hard for people to get obese. If you think it is easy, check this documentary of people trying hard to get obese.
7. What about people who gain a lot of weight as shown in NHANES study in US?
This is a good point. For people who are already heavy (around obese), the toxic environment is making them worse. And Karky had commented on this. They are gaining 3-4 times the weight than the normal or underweight people. These are the same people who make the average weight gain on US go up and make the rest of us look fat too. This is a classic example of gene-envronment interaction.
8. This kind of gives people a cop out in that it justifies the genetic component, but it’s a bit like saying “Cancer runs in my family, all of the smokers died from it.
There are number of people on Facebook and other blogs that have made similar comments. When did we get so concerned about their health and welfare I ask? Give them a break for heaven sake.

Most obese people are often depressed, lack self esteem and live a life in an endless cycle of self-blaming. There is no other population that has been discriminated for so long, even in the 21st century. These people have been discriminated and judged everywhere, in schools, workplaces, and even by health care professionals. It is clear in research that even health professionals (also people who treat obesity) associate obese people with being “bad” and “lazy” and “worthless”. This is largely because we still think obesity is all about a personal choices and we are too cuddled up in our cognitive biases to question our assumptions.
And for all the normal people who are crying out loud, why can’t you all get a six pack? After all just like losing weight, getting a six pack is as simple eating less and working more.
9. So you are saying just lose 10-15 lbs or 5-7% of the weight?
Losing weight is extremely simple in principle, but extremely hard for the majority and maybe almost impossible for some. And this is what the research says too. IOM (Institute of Medicine) and the NHLBI (National Heart, Lung, Blood Institute) recommends this too. In fact “success” in weight loss treatments is a weight loss of >=5% of bodyweight maintained for 1 or more years.
This amount of weight loss will not bring many people even close to normal BMI. Then why it is set so conservatively? Because we know that majority of people regain almost all the weight back within 3-5 years. The IOM summarized the long term findings by saying” those who complete weight loss programs lose approximately 10% of the body weight, only to regain two thirds back within a year and almost all of it back within 5 years”. And this hasn't changed a bit even now.
We have number of studies to show that even moderate looses have significant health benefits. In fact, two of the the large multicenter trials - the DPP and the LOOK AHEAD study- has shown this.
So lose 10-15 and maintain it for 6 months. If it can be maintained without extreme difficulty, try to lose more. I am not going to sit and argue with people who want to lose more. But they should understand what they are dealing with and be better prepared.
9. People could become fatalistic in their approach to weight loss upon reading the article.
Does anyone here have a better option?
What are you goona to tell them when they fail? And most will. That since it not genetics, it is probably you; so try again. And you thoroughly deserve all the mental agony and suffering you go through and also the stigma associated with obesity?
10. Ok agreed it is largely genetics. It will not change the treatment of obesity since we cannot change genes.
Finally, everything comes down what we can do about it. I wouldn't have written this series if there were no practical applications. Just understanding the biological basis of obesity, changes everything: It changes the way we treat obesity and treat obese people.
Note: If you want to learn more about this topic, start with this recent presentation about Friedman about the biological basis of obesty. He discovered Leptin. The book Rethinking Thin: The New Science of Weight Loss—and the Myths and Realities of Dieting by Gina Kolata talks about the same too.
Related Articles
The Cause of Obesity - Part 2
January 14 2012
In the first part, I come to the conclusion that obesity is largely dictated by your genes. I wrote about how your bodyweight is biologically regulated to be stay within a range, say 10-15 lbs. As I expected, and as you can read from the comments, many didn't agree.
There were a lot of comments, but the most sensible counter argument is how can there be an obesity epidemic if it is largely genes? Hence it is rather clear that obesity is largely due to our environment. And this is the argument almost all studies make to counter the biological basis of obesity. Here I am going to drill down further into the data and show exactly what these numbers mean and why is it is largely your genes.
How is obesity defined?
BMI: Obesity is defined by an index known as Body Mass Index (BMI). BMI is a crude measure of body fat based on just your height and weight. As shown in the picture, If you are between 25 & 30, you are overweight, and if you are over 30 - you are obese.
Why is it called an 'epidemic'?
Obesity trends: As shown in the figure above, if you gain weight to cross the 30BMI mark, you are clinically obese.
In the 1980's and 90's, as shown in the graph from CDC, a lot of people (20-74 yrs) gained weight and moved into the obese and extreme obese category. This is shown as a steep rise in the obese and severely obese lines in the graph. If you calculate, it shows a 33% increase in obesity and a 67% increase in extreme obesity in the 90's compared to the 80's. This sharp increase in the percentages prompted the researchers to call it an epidemic.
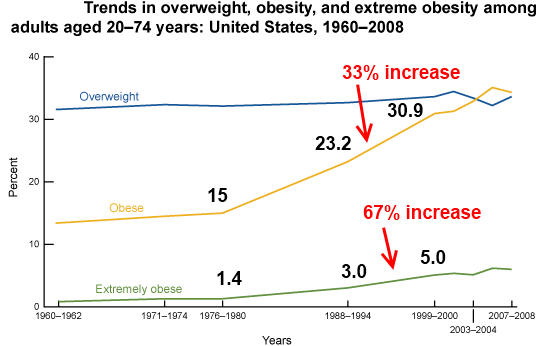
This was the same for childhood obesity too. For the age group of 6-11 there was a 73% increase and a 100% increase for the age group 12-19.
These numbers are huge and gives a picture of people all over in US just gorging on food and lying around doing nothing but getting fat.
How can this be an example to support the argument for genes?
The average weight gain is very modest: Though the percentage increases looks huge, the average weight gained is very modest. For example, there was a 33% and 66% increase in obese and extremely obese in the 90's compared to the 80's, prompting the term obesity 'epidemic'. But, in fact, the average weight gain was 6-8lbs in a decade! Of course, 6-8 lbs is important, but 6-8lbs pounds increase paints a completely different picture than the 33% and 66% increase which caused the 'epidemic'.
The weight gain is non-uniform and is even smaller for the majority: If it was environment, everyone including normal weight, overweight, obese and severely obese should have gained equally. But this is not at all what we see. What we see is a small increase in weigh for the majority, but very large increases in weight for the obese and severely obese. This can be seen in the graph which is skewed to the right.
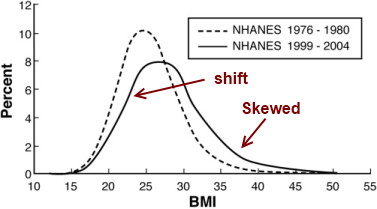
It is hard to tell this difference from the frequency curves. They are in fact smoothed (curve smoothing) to give those clean curves. The researchers hence used mean difference plot technique to look at the increases in weight based on the BMI levels. What they saw was less than 6-8lbs (1 BMI) increase for the people in the lower BMI catgeory, while almost 3-4 times this amount for the obese and extremely obese category. This graph for 30-39 year olds men (1976-80 till 1988-94) shows the general trend n the MD plots, though the differences are smaller in certan subgroups. This shows that even the average weight of 6-8 lbs in a decade is is largely due the obese and extremely obese category ganng weight. So people who are at normal or overweight BMI might have increased an average of 4-5 lbs at the most in the 90's.
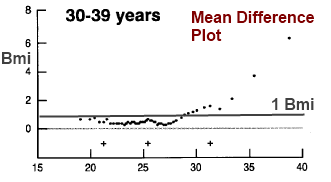
Ths clearly shows that for folks who are genetically predisposed to obesity, the toxic environment seems to make it worse. For people who are not genetically predisposed, the very same toxc environment is not making any big difference. Why is that?
Why do the weight gain and the obesity percentages looks so different? This is what happens when you give a cut off value to a continuous variable, like BMI. As you can see from the BMI graph, the majority of people are around the 25-30 BMI, so a small increase in weight will push a large number people from this area over to the obese category. This gives the impression that people are gaining a lot of weight.
What about childhood obesity?
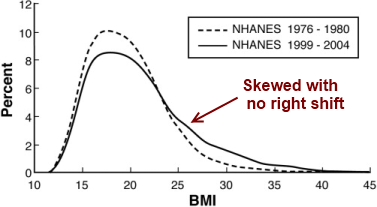
BMI: For childhood (and adoloscent) obesity, the increase in BMI is one-sided (see the skewed curve with no shift). Kids in the normal weight category hasn't budged, whereas the overweightand obese kids have gained a lot of weight. The increase in obesity for children is almost entirely due the heavier kids getting more obese.
How would the graph be if it was largely environment?
Environment: If it was largely environment, everyone would have been equally affected and would have gained a lot of weight. The curve would have shifted to right a lot with no skewness. This will show that there is no overriding factor for obesity. Everyone will get really fat!
What if we lower the calories and increase physical activity?
If we lower the calories and increase physical activity, the obesity trends will come down. The curve will be shifted to the left and less skewed; there will be less obese people, and obese will be less obese. But the shape of the curve will remain the exact same as in the 1970. That simply means there will be still obese people and lean people! And why is that? The short answer is 'genes'.
Practical Recommendations
Reference 1 | Reference 2 | Reference 3 | Reference 4 | Reference 5
NOTE: I first read this from Jeffery Friedman. Friedman discovered leptin which is the greatest discovery in nutrition. He even confrims his hunches about the modest gains of weight (and how these weight gans influenced by the heaviest people) from Kathryn FLegal. And who the heck is Flegal? Flegal is the lead author who publishes all the obseity prevalance data of US. Her papers are the very paers which we uses to show the increase in obesity prevalnce in recent times. I urge everyone to look into this topic closely than base your arguements on personal memmory and observations.
Related Articles
The Cause of Obesity
December 23 2011
Are obese people fat because they are lazy or because of their life style or their genes?
Now there is more and more evidence to suggest that obesity has a powerful genetic component and the cause of obesity is largely genetic. Apparently, there is a powerful unconscious biological system that is constantly trying to keep your body weight within a certain range, say with 10-15 lbs.

What is the evidence that obesity is largely genetic?
Animal Studies: Animals which are tube fed, voluntarily eat less. When the tube is taken off, they voluntarily eat more and get back to the previous body weight. Animals that are restricted food, lose weight. But they quickly get back to their previous weight when food is re-introduced. Why?
It appears as if the animals were looking in the mirror and badly wanted to get back to their previous weight.
Adoption Studies: Obesity is said to run in the family. The usual retort for this case is that kids brought up in the same obese family are exposed to the same environment and hence not an example for the genetics for obesity. However, adoption studies clearly show that the adopted children's weight more closely resembles the biological parent than the adopted parent.
Twin Studies: Identical and non-identical twin studies are mainly used to study the genetic contribution for a particular trait like height, cancer, heart disease and so forth. Identical twins (Monozygote) have almost exactly the same genetic make-up. Non-identical twins (Dizygote), on the other hand, share about 50% of the genetic traits. It has been shown from twin studies that percentage of heritability of obesity ranges between 70 % to 80% - the only trait being higher than obesity is your height! See the picture below.
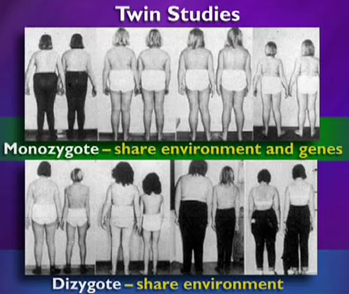
Hormones: The recent discovery of leptin, ghrelin, bombesin and other appetite regulating hormones now offer a mechanistic explanation for how our body weight is so tightly regulated.
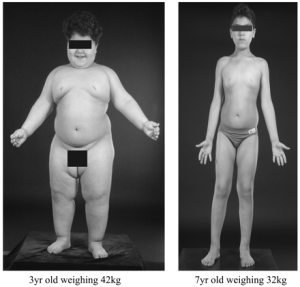
Leptin Gene: Mutations in leptin gene, leptin receptor have shown to result in massive obesity. Mice with mutations in ob gene (leptin gene) fail to produce leptin and show a fivefold increase in body fat compared with normal mice. An as expected, these are remedied with leptin treatment. Unfortunately, majority of obese seems to be resistant to leptin. So injecting leptin to treat obesity didn't live up to the hype.
Stability of Weight: As most of us have experienced, our body weight tends to be pretty stable throughout the year. According to the laws of thermodynamics, you will stay at the same weight if you match your energy intake to energy expenditure. That means, you somehow managed to spend exactly a million calories to match the million calories you ate throughout the year!
Over a decade, people gain 10 pounds or so. This small increase means that you have precisely balanced tons of calorie intake and output to a precision level of 99.6%. This is almost impossible for even the most ardent calorie counter since most calorie count on food labels are off by 10% or more!
Extreme Variations: Environment is always blamed for obesity. If that is the case, why are extreme variations in fatness within the same fattening environment? Are all the lean people who live in the same environment watching their diet throughout their life?
In twin studies, it is very clear that for the same calorie intake and expenditure, people lose different weight. In one study where identical twins ate the same amount of calories in a controlled environment, the variation ranged from 12llb to 28 lb! So it is not always obese people eating more food.
Dieting: It is now pretty clear that 75-90% of the people who lose massive amount of weight (50-100lb) gain most of it back within 1-2 years. It has been shown that when people lose weight, they not only feel hungry but that they also burn fewer calories than a person who is lean. The more you lose weight, the more the biological drive to gain the weight back.
Bariatric Surgery: Bariatric surgery is the most successful weight loss treatment. Bariatric surgery results in 20-40% initial weight loss; the majority of which is maintained for 15 years. It is now clear that bariatric surgery do not just work by making the stomach smaller. If that was the case, people could easily eat small frequent meals and get back to their weight; but they don't.
It has been now shown that bariatric surgery cures most people of diabetes. This cure happens a few days after surgery and even before they lose substantial amount of weight. Bariatric surgery seems to change the gut biology to the extent that it somehow resets the homeostatic mechanism that controls body weight.
If it is mainly genetics, why is obesity on the rise?
And this is the main arguement against how obesity is largely genetics. Genes don't change so fast so how can obesity prevalanace increase? So it is mainly the environment - they say.
BMI: Obesity is classified based on Body Mass Index. BMI is measure of body fat based on your height and weight. If you are above 25, you are over-weight; 30 and above, you are obese. This means that a small shift in bodyweight is enough to push a lot of people over the BMI category of obesity.
In 1999 a 33% increase in obesity was reported compared to the previous decade. In terms of body weight this just means a 3-5 kg increase in body weight. The 3-5 kg increase in bodyweight gives an entirely different picture than when you hear about a 33% increase in obesity!
Also the BMI of people between 15 & 30 hasn't changed much. What is going up is the BMI of people who are around 30BMI & over. The obese people are gettng more fat and making it look like everyone is getting obese, when it is clearly not the case.
What about the role of environment?
Gene-Environment Interactions: There are certain high risk groups such as the pima Indians and Pacific Islanders who have genes that are very susceptible to obesity. Pima Indians have an extremly high rate of obesity. For people who already have the obese genes, environment plays a permissive role. Environment is necessary, but not sufficient for obesity.
Overweight: For people who are moderately overweight like the majority, environment does play a role in the 5-10 lbs they gain over decades.
What about people who lose a lot of weight and keep it off?
These folks are clearly the minority, around 5-10%. It is not exactly clear how they do it. There might be a subset of people whose conscious motivation can override their biological drive in the long run. Majority of the people can’t.
Practical recommendations
1. We should focus more on health than weight or the cosmetic aspects.
2. It is clear than moderate weight loss of 10-15 lbs of weight loss in obese people can have dramatic improvements in their health.
3. It is also very clear that eating healthy and exercising has a beneficial effect on health independent of the change in body weight.
4. The major cause for obesity is your genes and not the lack of will power or lifestyle.
5. Obesity is not the fault of obese people. So treat them with respect.
Here is part 2: The cause of Obesity- Part 2
Related Articles



Is Exercise the Magic Pill?
December 04 2011
This was the title of the presentation I gave a week back. If you know anyone who doesn't exercise, send this to them please. Everyone kind of vaguely knows that exercise is important, but they got no clue about the breadth and depth of the benefits we are talking about.
Heart Disease: Heart disease is the leading cause of death in United States. Almost 300,000 people die of heart disease every year. In short, 1 out of 3 people would die of heart disease.
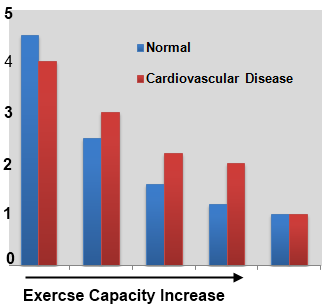
Exercise Beneifts: Number of observational studies have shown exercise to cut the risk of heart disease and the risk of deaths from heart disease by almsot 50%. Exercise capacity has shown to be a stronger predictor of death than established risk factors such as hypertension, smoking, and diabetes. As shown in the graph, it is now clear that as your physical fitness (exercise capacity) increases, the risk of dying decreases in a dose-response manner in both healthy and people with heart problems(1,2).
Cancer: Cancer is the second leading cause of death in USA. 1 out of 4 people would die of Cancer. 1 out of 8 women will be diagnosed with breast cancer.
Exercise Benefits: There is strong evidence to show that exercise may decrease the risk of colon cancer by almost 50% and breast cancer by about 30% from observational studies. Colon cancer is the most common form cancer in both men & women. And there some evidence to suggest that exercise lowers the risk of endometrial, lung and prostate cancer. Exercise has shown to lowers the risk of cancer recurrence or death in colon, prostate and breast cancer survivors too. It also improves the quality of life and lowers fatigue in cancer patients(3).
Diabetes: Diabetes is the 7th leading cause of death in the states. 1 out of 13 people would die of diabetes. Diabetes is the leading cause of amputations in the country.
Exercise Benefits: Number of observational studies & experimental studies have shown to cut the risk of diabetes by almost 60%. Exercise is also beneficial for treating diabetes. The famous study - Diabetes Prevention Trial - showed that exercise and diet cuts the risk of diabetes by almost 60% compared to the most popular diabetic drug- Metformin, whiich showed a 30% reduction(4).
Osteoporosis: Osteoporosis is the loss of bone density which can lead to bone fractures. 1 out 5 women over the age of 50 will develop osteoporosis. 1 In 5 women over the age of 75 who sustains a hip fracture will die within the next 2 years. Half of the survivors will end up dependent on others.
Exercise Benefits: Exercise, especially weight bearing exercises can be beneficial to prevent and treat osteoporosis bone density. It seems like we need more high quality studies to quantify the effect of exercise on osteoporosis.
Cognition: Cognition is just a big word for mental processes like memory, learning, attention and so forth. Recently, there has been an intense interest in the benefits of exercise on brain cognition.
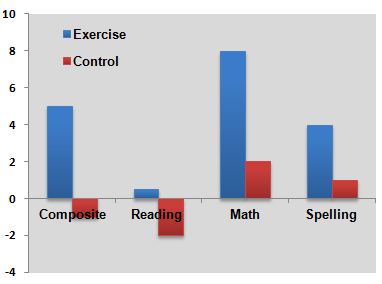
Depression: 1in 10 adults are affected by depression. Women are almost 70% more likely than men to suffer depression. Half of the deaths due to suicides is attributed to depression.
Exercise Benefits:There are 2 studies which show that exercise is as effective as anti-depressant drugs in reducing depression in people with mild to severe depression. The study also showed that exercise reduces the chances of the depression returning. After 6 months, only 8% in the exercise group relapsed compared to 30% in the drug group. It is safe to say that evidence is only suggestive and we need better quality studies to show a conclusive evidence of exercise for depression (8,9).
Side Effects: The side effects of exercise are almost zero, if done properly and gradually. It is typical for doctors to carefully evaluate to see if the side effects of the drug exceed the benefits of the drug. Just like exercise, aspirin works well to prevent heart attacks, but the side effect is cerebral bleeding.
I didn't really talk about the effects of exercise on obesity, treating pain, and preventing the loss of muscle mass since most people are aware of it. I also talked a bit about the minimum exercise required for achieving these benefits. Exercise research is still in its infancy; there will be more and more studies looking at the effect of exercise on other health conditions in the coming years.
Conclusion
Is there any pill out there which can prevent and/or treat so many major diseases, improve quality of life, has almost zero side effects, and costs almost nothing?
One hand went up in the crowd. A bit perplexed, I asked, “which drug is that?”
She said, 'exercise' - with a smile.
Reference 1 | Reference 2 | Reference 3 | Reference 4 | Reference 5
Reference 6 | Reference 7 | Reference 8 | Reference 9
Related Articles

Why is it Hard to Maintain Your Lost Weight?
November 27 2011
We know that 80% of the obese & overweight people who lose weight, gain most of it back within a few years. Is it because they lack the discipline or is there physiological mechanisms beyond their control that is driving the weight back.

It is now clear your body weight is regulated by your brain. There are numerous hormones in your body that controls your appetite to keep your body weight within a certain range.
Leptin: Leptin - one of the most important hormones- is primarily produced from fat cells and its circulating level is directly proportional to body fat levels.
Ghrelin: Ghrelin is released from the stomach and its primary purpose is it stimulates hunger,
Cholecystokinin(CKK): CKK is another intestinal hormon which suppresses appetite.
Eating less causes profound reductions in energy expenditure,leptin, cholecystokinin and increase in ghrelin and appetite all of which promote weight regain.
What was the study purpose?
The purpose of the study was to see whether these fluctuations in these appetite regulating hormones persists with prolonged maintenance of reduced weight.If it persists, it maybe be one of the reasons why people gain back weight so easily.
What was the sudy design?
The study involved 50 overweight or obese participants in a 10 week weight loss program. They measured different hormones and appetite levels before the weight loss, after the weight loss (10 weeks), and after 62 weeks of weight maintenance.
What were the results?
The mean weight loss was around 26 lbs after 10 weeks. There were significant changes in hormones and appetite after weight loss, and all these changes persisted even after 62 weeks.
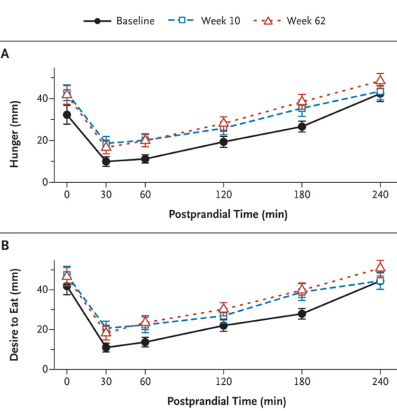
The raph shows how hunger and 'desire to eat' were significantly higher after 10 weeks and 62 weeks compared to baseline. In short, it just means that your body is trying to get back to the baseline weight.
Conclusions
There are multiple compensatory mechanisms vigorously resisting weight loss in obese and overweight people.You didn't gain the weight back just because 'life got busy' or you lacked the will power.
Related Articles
ACE Fitness Conference 2011 Review
November 13 2011
The American Council of Exercise (ACE Fitness) conference 2011 was held in San Deigo on Nov 2-5. I had ACE certification years back and this was my first ACE symposium. Here are some of the presentations which I thought were interesting.

Thomas Plummer
The keynote presentation titled “Changing lives .. Creating a Fitness Career that matters” by Thomas Plummer. He founded the Thomas Plummer Company and the National Fitness Business Alliance (NFBA). Plummer speaks to more than 10,000 people each year through engagements as a keynote speaker, workshop host and private consultant.
This was a good one. He talked about where the fitness industry was, where it is now and where it is heading towards. The topic was very relevant and he communicated his points really well, I thought.
He talked about the end of traditional training model which was based on the training philosophy of the bodybuilders in the 1980's: the circuit machines and the steroid bodybuilders. It was all about lifting heavy weights, using machines, single joint exercises, crunches, and long cardio sessions, and low fat, high carb diets. The fitness field is moving more towards full body, functional, multi-joint than the one day a body part, single joint exercises bodybuilding model.
I agree with most of what he says. And I have wrote in the past how the majority of what bodybuilders do do not apply to the majority of the people who go the gym. The recent article I wrote about the lat pulldowns is an example of this. We are taking a model which may be good for a bodybuilding population and applying to a completely different population whose goals, priorities, motivation levels are completely different.
And as I always say it always goes back to client goals and preferences. If someone wants to get muscular, it is always better to focus on multi joint exercises, lifting heavy, with a few isolation exercises here and there than just working with ropes, medicine balls,TRX and other functional movement stuff all the time. You can also throw some functional stuff at the end to spice up the workout for your client. You don't have to look at it as an either or situation which is what most people tend to do.
Another good point he talked was the failure of the big box model clubs with lines of circuit machines , ab area, and personal trainers. The new generation club are much smaller,circuit lanes are replaced with functional cable machines, they carry a few dumbells, a few squat racks, a floor area with number of fun tools like kettle bells, medicine balls, bosu balls, ropes, sled pushing, a few treadmills and ellipticals,and group training instead of one- on-one training. This is true and I see these small facilities popping up everywhere. This is basically the Crossfit model which has gained so much popularity these days.
But I am not sure if this is entirely true because places like Planet Fitness, 24 hour, Lifetime are just the typical box model types and they are all just growing. For example, Planet fitness has around 400 to 500 fitness centers in US with around 5K-6K members and almost 95% of them are making profits. Planet fitness does not have contracts and their memberships are around 10-15 dollars. Compare this to an average gym which makes you sign contracts and makes you pay around $49 a month!. Now get this, they have machines, and they also have a designated circuit machine workout area with lights to time your circuits!
He talked about some other few points but I forget. And I am yet to see the presentation slides that the ACE people told they will upload to the website in a few days. Talk about customer service …
Todd Durkin
Todd Durkin, MA, CSCS, is an internationally recognized performance-enhancement coach, personal trainer, massage therapist, author, and speaker who motivates, educates and inspires people worldwide. He is the founder and creator of Fitness Quest 10 & Todd Durkin Enterprisesin San Diego, CA. He is a 2 Time Personal Trainer of the Year (IDEA & ACE) and has received numerous industry accolades
Todd is an excellent speaker and is very motivating and energetic. He was like a Bull on red bull. Hs presentation was titled the “The business of personal training”. It was just an overview about how to make your personal training business better or in his words - 'world class'. He had a lot of good points about how to motivate your clients and your team, but nothing really that I wasn't aware of. If you are really customer focused, if you really want to improve, you would come across these.
I wish the content was a bit more organized, and also he didn't skip content in the slides. Every time when I see presenters skipping content and slides, I just think they didn't care enough to make changes or rehearse it. He gave a lot of good tips and books to read throughout. But I like to focus on concepts and big picture rather than tips. They are like those typical Muscle & Fitness articles like '5 Tips to lose weight or a stronger bench'. If you cannot see the underlying concept, you will be like one of those 16 year old's waiting for the magic bench program in the next Muscle & Fitness edition. Todd was nice enough to raffle out free DVD's and books which I thought more presenters should do than just send a paper around to get people's email addresses.
Michol Dalcourt
Michol Dalcourt is an educator, author, trainer, inventor, and an industry leader in the areas of human movement and performance training. is currently an Adjunct Professor at the University of San Francisco in the Faculty of Sports Science, Director of the Institute of Motion, and Co-Founder of PTA Global.
The tile of the presentation was “Correcting Dysfunctional Movements”. I know where this was going, but I wanted to say what he had to say and if there is anything new. After 20 min of going an exercise of finding joints which are primary and secondary, he went to show some slow, one- legged exercises which was suppose to make your foot pronation right. Somebody who was really smart asked if can we indeed change the foot dysfunctions and as they all say he replied “you can do it, but it will take along time”. Sure if it doesn't work, you didn't do it long enough or you didn't do it right! He also made sure he had some biomechanical explanations for every little twist and degree change you do with the exercise. And I am guessing he did this for every major joint, but I didn't wait for that long.
People always say research is mumbo jumbo. Research is pretty simple. You take a group with back pain or knee pain, make them do exercises to fix pronation or whatever and show that as their pronation improved, their knee or back pain improved compared to a control group. This is the basis of randomized controlled studies (RCT) in research which is the gold standard of finding if a drug or treatment works. They don't care about the biomechanical mumbo jumbo or your rationale for doing the exercise. And the whole correcting movement dysfunctions or posture or FMS field is lacking these basic RCT's. Even the shoulder scapular dysfunction studies show decrease in pain with scapular exercise, but the scapular dysfunction remains the same. There are people with scapular dysfunctions who have no pain and people with no dysfunctions have pain. What does that tell you about 'dysfunctions'?
I went to a few more , but it was mainly group fitness ones and activity type classes. I just wanted to get better at it so that I can train my instructors. You guys wouldn't be too interested in those stuff anyways. ACE fitness conference I felt was more about the 'How' than the 'Why' like at the NSCA conferences. That’s all I have.
Related Articles

Can Circuit Training Increase Strength and Muscle?
October 30 2011
Circuit weight training takes less time compared to traditional weight training, but can it increase strength and muscle similar to a traditional routine?

What is circuit training?
Circuit Training: This type of training involves lifting lighter loads with very short rest periods of time. The lifter moves from one exercise to the next in 15 -30 sec (or no rest) and completes a series of circuits. The weight is usually around 40-60% of 1Rm which equates to 10-20 reps.
What are the advantages of circuit training?
Cardiovascular: There is a moderate Increase in cardiovascular capacity compared to traditional strength training.
Time: Less time is required since there is little or no rest in between sets.
Fat Loss: There maybe greater fat loss with circuit training compared to traditional training.
What are the drawbacks?
Strength & Muscle: Since the weights used are pretty light, the strength and muscle gains are minimal compared to traditional training.
Bone Mass: This is also true for bone mass since there is less loading.
What was the purpose of the study?
Purpose: The purpose of the study was to study the effect circuit training with heavier loads ( 6 reps) on body fat, strength, muscle, cardiovascular response compared to a traditional routine.
What was the training protocol?
Duration: 8 weeks
Participants: The subjects were trained men.
Rest between sets: The traditional group did the same number of exercises separated by 3 min rest while the circuit training group rest time was 35 sec.
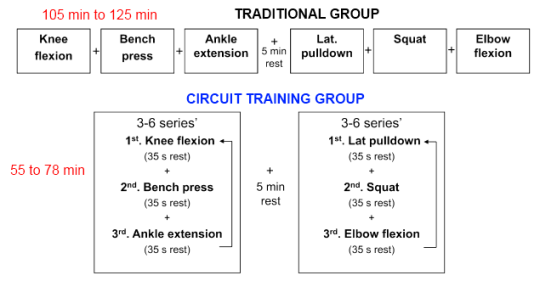
What were the results?
Practical considerations
Related Articles


Braden Sowle - Natural Bodybuilder Interview
October 19 2011
I know Braden pretty well. Braden has worked for me for almost 4 years now. We always have a lot of interesting conversations about diet and training. Braden’s whole life is all about bodybuilding – he eats, sleeps and drinks bodybuilding. Braden is pretty humble and always willing to help anyone who has questions about their training and diet. Braden is currently working on his M.S in Dietitics.

Age: 25
Competition Weight: 175-185.
Offseason Weight: 205-212.
What is your training program?
It’s hard to describe since it changes so often… a good program is progression based, is dynamic and changing, involves some heavy lifting for dense muscle as well as some higher volume training for that fullness and roundness. I am between competitions right now so I’m just trying to maintain intensity, prevent injury, increase fullness, and most importantly improve conditioning by burning some fat.
What is your diet like?
I eat different everyday depending on my activity levels. But overall I eat a wide variety of foods similar to what our ancestors ate avoiding most pre-packaged and processed foods while focusing on quality sources of meat, veggies, fruits and nuts.
Protein sources: Egg white, whole eggs , turkey, cod (other white fish), salmon, beef(venison or buffalo) whey protein isolate/conc/hydro
Carbohydrate sources: Sweet potatoes, Brown/white rice, oats, sugar free carbohydrate powder
Fats: olive oil, almond, pecan, walnut, peanuts (technically considered a legume)
Fruit: blueberries, raspberries, pear, nectarine, peach, cranberries, apples, lemon, pineapple, plum, etc..
Veggies: Broccoli, Asparagus, Green Beans, Spinach, Romaine lettuce, peppers, onions, mushrooms, bok choy, etc…
Dairy: Greek yogurt
Supplements:
(fat burning) - Caffeine, beta alanine, l-carnatine , green tea.
(strength, power, recovery) - creatine BCAA (recovery), glutamine.
(Increase blood flow) - Arginine.
(Joint lubrication/repair) - glucosamine(w/msm}+chondroitin.
(promote healthy hormone levels) - Vit D, vit E, Zinc fish oil, flax oil.

My eating schedule depends on my activity level, eating more on harder workout days. Each meal has a significant source of protein, and either complex carbs or veggies depending on the timing, I eat most of my carbs in the two meals before my weight training session. On my rest days I eat less carbs and calories.
What do you think are the 3 most important things that people who want to get bigger should focus?
Chips, pizza and ice cream ……but that’s if you want your waistline bigger.
If you want the growth to be muscle mass
1. Design a training split with enough recovery for each body part
2. Be patient, Rome wasn’t built in a day!
3. Don’t make excuses! - Anyone can get bigger you just have to eat more and lift more than you are currently.
Do you think there is a difference in training of natural bodybuilders and bodybuilders on drugs?
Natural athletes need more recovery and I believe in using very low and very high rep ranges to shock the muscle into growth. Most steroid using bodybuilders seem to grow using the traditional 8-12 rep range. Let’s say you dead lifting, rather and doing 3 sets of 10 with 315 or 365, I’d recommends doing something like 495x2, and 405x14…
Do you think bodybuilders should worry about strength like power lifters?
Yes they should try to increase their strength, but not by any mean necessary like power lifters. A bodybuilder who wants to build a bigger chest may try to increase their bench, but if they use their delts and triceps instead of their chest to do the work - the wrong muscles will grow.
What do you think about the low volume and high volume approach of training?
I’ve had success with both types of training; I think rotating between high and low volume programs is best. When I diet for a competition I reduce my volume a bit, but I try to keep my strength and intensity as high as possible.

What are your future goals?
I’m a big believer in short and long term goals. My short term goals include finishing school and earning my pro card as a natural bodybuilder. Long term I want to work with professional athletes as a Strength/Nutrition coach.
What are the 3 biggest mistakes people make in the weight room?
Not training with enough intensity, not emphasizing sleep and nutrition enough, keeping form too strict when it comes to getting bigger, “if you ain’t cheatin’ you ain’t tryin”.
If you have any questions for Braden, ask in the comments please. Thanks Braden and good luck with everything.
Related Articles

Do Power Balance Bracelets or Bands Work?
October 10 2011
Power balance bracelets have become wildly popular in the last couple of years. There are dozens of professional athletes, celebrities and musicians wearing these, and some even endorsing these bracelets.
So what are Power Balance bracelets?
As the name suggests, these are just ordinary rubber bracelets made in China. What makes it stand out is they have embedded these bracelets with holograms.
They come at an 'affordable' price of $29.99.
What are the Power Balance bracelet claims?
Hologram: The hologram on the power balance band is supposed to interact with your body frequency and it supposedly reacts differently for different people. Also according to the website, “The thin polyester film hologram is programmed through a proprietary process, which is designed to mimic Eastern philosophies that have been around for hundreds of years.”
Performance: Before thy got sued for false and misleading claims, they advertized power balance to increase strength, power and flexibility by 500% and called it performance technology. Now they cleverly word it as “maximize their potential and live life to the fullest.”
Testimonials: There are lot of testimonials from professional athletes about how power balance bands has helped improve their performance and they just can't take it off now.
Does Power Balance bracelet work?
Nope.
Then why do people think it works?
There are no scientific studies showing that power bracelet balance works. And there is no earthly science even remotely saying that we can capture frequencies and bottle it in a hologram. Then why do some people feel or think it works?
Placebo Effect: If you believe or expect a procedure or a pill to improve you health or behavior, it will. Apparently, the pill or procedure do not have anything to do with is improvement. Watch this cool video about placebo effect.
Flexibility: Power balance band test involves a flexibility test where you try to stretch and reach as far as you can. And then they are made to repeat the stretch wearing the power balance band. This always works since now you have a goal to go beyond. People always do better the second time than the first one even if they wear a band or not.
Strength: Another test the power bracelet band use to have you stand on one leg and have your arm to the side. The sales guy then pushes down on your hand. Almost everyone falls off balance. After they wear the power band, no one falls off balance.
This is just basic physics being abused. The first time the sales person pushes down and out of the body which pulls you out off balance. The second time he just pushes down and 'into' your body which is not pulling you out of balance. This is what is shown in the picture.
Practical Applications
Related Articles
The Hallmarks of Cancer
October 02 2011
Cancer is different from other diseases because it is not just one disease, but a collection of more than 100 distinct diseases. If so, what are the commonalities shared by different cancers?
Picture: A breast cancer cell
In 2000, the journal Cell published a ground breaking article titled “The Hallmarks of cancer”. This paper has turned out to be the most cited paper in the cancer field. Below are these 6 hallmarks of cancer.
And if you are wondering about the topic, I keep up with most of the health-related topics. This site is not just about bench press and biceps. This topic is also a bit dear to me since my Mom passed away a year back after battling with cancer for almost 3 years. I have blunted the language a bit so that it makes some sense.
Growing out of control: Or Sustained proliferative signaling. Normal tissues carefully control the production and release of signals which control growth. But cancer cells have developed their own signals . They chose when to replicate and when to grow.
Evading growth suppressors: Just like there are signals to trigger growth, there are signals that suppress growth in normal cells. But cancer cells somehow are resistant or suppress these growth blocking signals.
Blood vessel growth: Or Inducing Angiogenisis. To sustain the growing size of the tumor, cells need a good blood supply to ensure enough oxygen and nutrients. Cancer cells activates the process of making new blood vessels(angiogenesis) to sustain themselves.
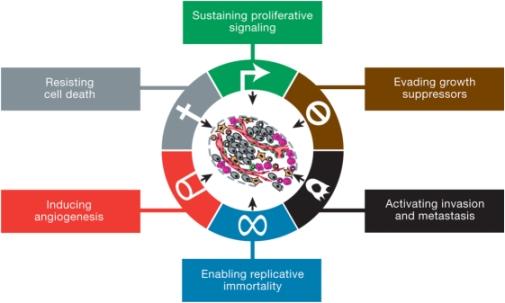
Evading Death: Or Resisting Cell Death. Normal cells are programmed to die or commit suicide after so many cell cycles or when they get damaged. It is called programmed cell death or apoptosis. It is a fundamental property of normal multi cell tissue. It is just another check to prevent abnormal growth. But cancer cells earn how to avoid cell death.
Invading other cells: Or Activating Invasion and metastasis. Most of the deaths from human cancers (90%) are due to cancer cells spreading and establishing colonies in other parts of the body. Cancer cells have learned to migrate to other parts in the body and invade healthy cells.
Unlimited copies: Or Enabling Replicative Immortality. Normal cells can only divide so many times, but cancer cells just keep dividing and making unlimited copies.
Journal nature had an article on how these hallmarks are common to even benign tumors (harmless) and hence cannot be called 'hallmarks'. The only hallmark not common to both benign and harmful cancer is the ability to invade other cells and metastasize.
Very recently, in March 2011, the authors updated the hallmarks by adding two more:
Cancer is a deadly disease, but it is most fascinating to learn and wonder about the intricacies of such an extraordinary disease.
Related Articles

Can Participating in Sports Make You Better at Everyday Tasks?
September 25 2011
Can cognitive skills attained through participation in sports transfer to your everyday life?It is clear that expert athletes outperform less skilled athletes in sport specific skills requiring attention, speed, perception and so forth.
But can these sport specific abilities transfer to every day multitasking activities like driving and talking on your cell phone?
What was the purpose of the study?
Purpose: The purpose of the study was to find if athletes can do everyday tasks better than non-athletes. It is assumed that participating in sports relates to multitasking and increased processesing speed that can carry over to similar tasks in daily life
What was the design?
Participants: The study recruited 18 Division 1 athletes and 18 non-athletes. The sport the participants played included baseball, gymnastics, swimming, tennis and so forth. Non-athletes were not involved in any university organized sports.
What was the outcome measured?
Street Crossing: A virtual reality street crossing task was used as the test. It involved crossing a virtual intersection while avoiding traffic.
Just to add some fun, they performed street crossing task under three distraction conditions-no distraction, conversing on a cellular phone with a hands-free device, or listening to music through headphones on an iPod.

The participants were instructed to walk and not run.
What were the results?
Atheletes better: The athletes showed statistically significant higher success rates (75% vs 50%) in crossing the streets reflected by fewer collisions with moving vehicles. This was also true for the distracted conditions too.
Other Studies: Other studies have confirmed that athletes perform better than non-athletes in laboratory testing of cognitive measures which includes processesing speed and tests of attention. As expected, athletes from interceptive sports like basketball, baseball, soccer showed the largest gains.
Practical applications
Related Articles




Understanding & Treating Pain in 5 minutes
September 05 2011
The video tells what 90% of people do not know about pain in less than 5 minutes!
Related Articles
The 4-Hour Body by Tim Ferriss Review
September 04 2011
The 4 hour body is a New York Best Seller written by Tim Ferriss. Before writing this book, he was just another productivity expert with a book called “The 4 hour Work Week” in the New York Best Seller List.
. Here is the 4 hour body review.
What are the claims in 'The 4 Hour Body'?
There are quite a few claims in his book, but I will review about this specific one: How Tim Ferriss gained 34 pounds of muscle in 28 days in a total of 4 hours in the gym.
Did Tim Ferriss gain 34 pounds of muscle in 28 days?
Muscle & Water : Before you start thinking about Tim Ferris’ four hour body workout routine and diet review , you need to understand what constitutes 34 pounds of muscle. Tim Ferriss says he used hydrostatic weighing for testing. Hydrostatic weighing is the gold standard of body fat testing. Most body fat and muscle measurements are 2 compartment models - means they only recognize fat and muscle. But the point here is that when it means muscle it counts muscle, bones and water. So when people say they gained 20 lbs of muscle, it not just muscle tissue, it includes water and bones.
Natural bodybuilders gain 15-20 lbs a day after their competition because they eat a ton and put all the water back and more. If we measure them with hydrostatic, it will show that they gained 20 lbs of muscle! Can you believe gaining 15-20 lbs of muscle in a day? And Tim Ferriss is not a newbie when it comes to body fat loss and water manipulation. From his blog” In 1999, I was a gold medalist at the Sanshou (Chinese kickboxing) national championships in the 165-lb. weight class (here is a video sample of Sanshou). This is perhaps the most controversial accomplishment in the 4HWW, as I make it clear: I arrived the on-site at 187 lbs., weighed in at 165 lbs., and stepped on the platform to compete the next morning weighing 193 lb.
Now tell me how hard is for him to gain 34 lbs in 4 weeks if he can lose 22 lbs of muscle and gain 28 lbs muscle overnight?
Muscle Memory & 4 Hour Body review: This is a physiological phenomena which makes it easier to put back muscle or strength that you lost . It means that if you stopped working out for a few months or a year, you can easily put that same amount of muscle or strength that you had in weeks. Tim Ferriss writes in the 4 hour body about how he had weighed 197 pounds in 1996 and was easily the strongest he has ever been. Also how he has gained 20 lbs in 4 weeks in aleast 4 occasions. This is totally different from a beginner trying to gain 34 lbs of muscle in a few weeks.
High Intensity Training & 4 Hour Body review: What program did he use in the 4 hour body? He basically used an HIT program which has been around for years. I really doubt anybody bothers about HIT anymore besides a handful of HIT experts. I am not going to write what exactly HIT is since no one really knows what exactly is HIT. Every HIT expert has their own version and their own science (and philosophy when they run out of science)to support it. For example, Arthur Jones prescribed 14-16 exercises solely using machines, Mike Mentzer took it to the extreme with 3-4 exercises for 10-14 days and Ellington Darden - Arthur Jone's assistant who is currently the modern voice of HIT - reccommends 7-12 exercise per routine, 2 days per week and includes both machines and free weights. Just to show how HIT experts make their own rules, Ellington Darden - the most famous of HIT experts - now recommends Not To Failure sets (NFT). This is called taking a complete u-turn in your philosophy considering the whole philosophy of HIT is based on 'going to failure' with just one set. Darden also thinks that most HIT enthusiasts have gotten carried away by prescribing very few exercises like 3-4 exercises and very low frequency like once a week. Tim Ferriss' workout uses 3-4 exercises and even goes to recommend once a week frequency further into the program. So who are we supposed to believe? Tim Ferriss who base his 4 hour body book writings on Arthur Jones or Ellington Darden who is the most famous HIT expert second to Arthur Jones?

The Colorado Experiment & 4 hr body review: And how was Tim Ferriss convinced that he could gain 34 lbs of muscle? He read about the infamous Colorado experiment conducted in May 1973 by Arthur Jones with a bodybuilder named Casey Viator (in picture). The claim is that Casey gained 64 lbs of muscle. Just remember that Casey Viator had almost dropped 33 lbs of muscle due to an accident and allergy, wasn't training for almost a year before the experiment, and was on steroids previously. Nobody has ever been able to replicate that much of muscle mass in a short period of time. I am sure someone will if they stop training for a year, had used steroids, and dropped almost 35 lbs of muscle before they started the experiment.
Science & 4 hour body: I love how the 4 Hour Body has a Chapter called “spotting Bad Science” at the end of his book. I whole heartedly agree with everything he had to say about the problems with observational studies, lack of control groups, the funders having vested interested and such. But I don’t understand how he couldn't find the reviews (atleast 2) which concludes that multiple sets are better for muscle (& strength) in both trained and untrained. I thought it was funny how he quoted just one study published in some online journal and writes how the author of the study incorporates '112 sources to answer the question', but then later we have chapters about spotting 'bad science'.in his 4 hour body book
Some of his diet rules like avoid fruit, milk and white flour like plague are just the typical fear mongering and bad science that most diet authors are known for. He writes that his 4 hour body book is a result of thousands of hours of 'jaw dropping personal experiments'. And I ask what makes his approach so different from other fitness experts and diet gurus? They all think it works for everyone because it worked for them, they all have a before after picture, they all have plenty of anecdotes & philosophy, and they all think that the conventional wisdom about diet and muscle growth is just dead wrong, and guess what they all get results in 4-6 weeks too.
The 4 Hour body book, the incredible claims, and the philosophy is no different from any one of those hundreds of diet and muscle books out there.
Related Articles

Hypothesis Testing & the Casey Anthony Trial
August 14 2011
Hypothesis testing is one of the most important concepts in scientific studies, but most people don't understand it. Atleast I didn't get it when I took my stats and research class. In this article, I will try to elucidate this concept by comparing it to the recent Casey Anthony trial
What is hypothesis testing?
Hypothesis Testing: Hypothesis testing is a method used to make a decision in scientific studies. It tries to figure out if a hypothesis is true based on probabilities.
Imagine you want to test if Drug A is better or not in lowering deaths in cancer patients compared to a Drug B. In hypothesis testing, you first come up with 2 hypotheses.
But why have two hypotheses to prove a single hypothesis?
This didn't make any sense to me when I was introduced to this concept.
If you want to show a difference, why just start with one hypothesis that there is a difference between the drugs and try to prove it? Why the heck should you come up with a hypothesis that there is no difference and then try to disprove it to show there is a difference? It seems counter intuitive to most people, but there is a good reason as you will see.
Popper's Theory: According to Karl Popper, one of the great philosophers, you cannot prove a theory, you can only disprove it. For example, let's say you want to prove a theory that all swans are white. This will be extremely hard to prove since you will have to go to every nook and corner of the world to make sure all swans are white. But it is extremely easy to disprove thee theory: You just have to find one black swan. And if you tried really hard and couldn't find a black swan, you support the theory that all swans are white (but , mind you, you didn't prove the theory since there might be a black swan hiding somewhere in the world) .
And hence the reason, you come with a hypothesis and then you try to disprove it. If you disprove it, you accept the second hypothesis or the alternate hypothesis. In hypothesis testing we use probability to disprove the hypothesis. Make sense?
Now what has this got to do with Casey Anthony?
Casey Anthony 's trial is a good example of how people don't understand this concept. For people outside US, Casey Anthony is a Florida woman who was recently acquitted of killing her 2-year old daughter. This was one of those murder trials which took the country by storm. Almost everyone thinks that she killed her daughter and she should have been punished.
 The whole hypothesis testing makes a lot of sense when we look at how the American justice system is set up. Just like in hypotheses testing, you come up with 2 hypotheses before the trial.
The whole hypothesis testing makes a lot of sense when we look at how the American justice system is set up. Just like in hypotheses testing, you come up with 2 hypotheses before the trial.
US Justice System: Just like in hypothesis testing, the lawyers try to disprove the hypothesis that Casey is not guilty. Instead of using probability, lawyers use evidence in form of DNA, witnesses and so forth. In the trial, the prosecutors couldn’t disprove the null hypothesis that she is not guilty with the evidence they had. So the jurors had no choice but to accept the null hypothesis that she is not guilty. Just like swan example, this doesn't mean or prove that that she is innocent.
A lot of people in the media were going crazy thinking how on Earth can the jurors think that she is innocent. But the jurors never thought she is innocent. One of the jurors put it best after the verdict- She said we never said Casey Anthony is innocent. This goes back to the concept of how you cannot prove a theory and we can only disprove a theory with the evidence in hand. The jurors understood this concept very well.
Related Articles

NSCA National Conference 2011 Review - Part 2
August 01 2011
Here is the second part of my review of the NSCA National Conference. To read the first part, click here

Dr. Dan Bernadot
Dr. Bernadot is a Professor of Nutrition and the Director of the laboratory for Elite Athlete Performance at Georgia University. Dan’s presentation was titled “Within Day energy Balance for Better Weight, Body Composition, and performance”.
Dr. Dan talked about the issue of meal frequency - how many times you have to eat in a day to improve body composition. From what I have read, eating more frequently do not raise your metabolic rate or improve your body composition, though every fitness magazine swears that eating 6-8 times a day raises your metabolism. So I was very interested in looking at his references.
His first major study was an observational study done on elite gymnasts and runners. The study was based on self reporting and showed that the larger the energy deficit (in both frequency and /or magnitude), the higher the body fat. Keep in mind that this study is based on self reporting, the correlation coefficient was less than .50, and was studied on a population notorious for eating disorders and menstrual problems. It is hard to conclude anything more than a weak association between the frequency of food intake and body fat from this study.
Now for an experimental study with a control group –at least that’s what I thought from the slide. But the study was just a poster presentation and never got published. And the study did not study the frequency of meals, it only looked to see if a caloric surplus affected body composition in athletes. And, as expected, it did in a positive manner.
In fact, there are a few studies which have showed increase in lean body mass (or decrease in muscle loss) with lower meal frequency compared to a higher frequency. But the studies used BIA to measure body composition. In short, it seems like we do not have any strong evidence to show that a higher meal frequency helps lose weight or maintain muscle mass better than a lower meal frequency.
The second part of Dan’s presentation involved a dietitian talking about meal plans and recipes and how you can ‘make’ your athletes eat 6 times a day. Considering how college students have a hard time finding time or motivation to prepare and eat meals, strong recommendations like these need some strong evidence to be justified. If you can control your appetite better with 3 meals a day and hate taking the time to eat 6-8 meals (and most do), there is no convincing data to tell you otherwise.
Dr. Jeffrey Stout
Dr. Stout is an Associate Professor and the Director of Metabolic and Body Composition Laboratory in the University of Oklahoma. Dr. Stout presentation was titled “Nutritional Supplement Approaches to Male Athletes”.
This was a good presentation: He had all the relevant studies and he narrowed his presentation from acute to long term studies. In the acute studies, he showed how a carb-protein supplement showed lower cortisol levels and lower muscle damage (creatine kinase). He also had some data showing how protein-carb supplement increase endurance performance, time to fatigue and decrease muscle damage. By the way, I am yet to see a endurance athlete talk about post workout nutrition.
For long term benefits, he showed a couple of studies which showed an increase in muscle and strength. He also talked about creatine and how creatine shows an increase in strength and muscle. It wasn’t anything ground breaking, but it was good to see someone lay out the evidence neatly.
I have talked about in the past that only the Cribb study directly supports the pre-post supplementation protocol to increase strength and muscle. There are two major reasons for this: In most supplement timing studies that I have seen, the participants were tested in the morning under fasted conditions. This is not how majority of people workout unless you are training in the morning on an empty stomach. Also, if we are studying the timing, the study design should be such that one group consumes the supplement Pre and Post and another group consumes it further apart from their workouts. But most long-term studies which looked at supplement timing used a control group that just had water or a carb solution post workout.
I would love to see a study with the same design as the Cribb study, but with a few changes: A placebo group so that the subjects who are in the pre-post group are not subjected to the placebo effects. In fact, a placebo group is required in drug trials if you are testing the efficacy of a drug. Also, a study performed by authors who have no financial ties to the supplement industry. It pretty clear now that favorable results are more likely in studies where there is a financial conflict of interest.
Related Articles

NSCA National Conference 2011 Review - Part 1
July 24 2011
National Strength & Conditioning Association (NSCA) is the world’s leading authority in strength & conditioning. They hold an annual conference every year which attracts conditioning & fitness professionals from all over the world. The conference includes presentations from leading fitness & conditioning experts, and was held in Las Vegas from July 6 till July 9, 2011. Here is the part 1 of my little review.
Dr. Stuart Mcgill
Dr. Stuart Mcgill is a professor of spine biomechanics at the University of Waterloo , Canada. His advice is often sought by governments, corporations, legal experts and elite athletes and teams from around the world. Difficult back cases are regularly referred to him for consultation.
Dr. Mcgill presented two topics. I attended the first and many people thought this was one of the best presentations. In the first presentation, he talked a lot of training concepts (titled ‘Lessons learned from the greatest athletes’). He talked about training the speed of contraction and relaxation, spending more time with asymmetric carries, learning to enhance stiffness in the core, avoiding spine flexion movements and so forth. In short, Dr. Stuart Mcgill’s work is basically about increasing performance and preventing low back injuries and pain largely by focusing on the core.
I was a bit concerned about how he makes so many absolute statements without too much evidence. When it comes to performance, I just think we are just over -emphasizing the role of core. Why are we so worried about the core? Has it been shown that just like strength, endurance, vo2 max, vertical jump and other proven variables, core strength is a major determinant of performance? No. Has it been shown that improving core strength can improve performance? No. Is there a general test for reliably measuring the core strength? No. So when Dr. Mcgill says that the great athletes fire this particular core muscle more than the others(or in a particular way) and hence we should all train that way, I would say that’s just another correlation. I just didn’t see many studies from him to support his statements either.
If we really want to say that this particular observation is really important for performance and it is what makes great athletes great, we need to do an intervention study. Find athletes from different disciplines, put them through his intervention, and show how they increased their time or distance or speed or strength and so forth than the control group.
When it comes to low back pain, I think it is pretty clear that the psychosocial component is very important, and maybe even more important than the biomechanical aspect. I have never heard or read Dr. Mcgill mentioning the psychosocial factors involved in pain. Even American College of Physicians recommend not to scan people with non-specific low back pain because what you find on a scan has very little to do with the onset, severity, prognosis, or duration of low back pain. Considering the bulk of evidence against the biomechanical model of pain, I think it’s a bit perplexing (and bothering) that he doesn’t even bother alluding to it and keeps ignoring it. Dr. Mcgill’s studies are a good example of studies which measure surrogate measures like EMG, spine models, compressive/shear stress instead of looking at meaningful outcomes to people like pain, performance or strength. There is nothing wrong with these studies, but you have to be careful about extrapolating your conclusions because you might be very well wrong. If you are not sure what I mean by surrogate measures, check my recent post on it.
I couldn’t attend his second presentation, but he seems to have changed his topic of his presentation because the presenter before him talked about how we don’t have much evidence about what causes low back pain or how to treat it. Unfortunately, it is true, and Dr. Mcgill disagreed to the extent that he felt he should change his presentation. If he had enough studies to show against, he wouldn’t have to talk so loud and so often and talk about so many anecdotal evidences, I thought.
Dr. Chad Kerksick
Dr. Kerksick is an Assistant Professor of Exercise Physiology and Director of the Applied Biochemistry and Molecular Physiology Lab at the University of Oklahoma. Chad talked about Intensity vs volume in muscle growth. Chad spoke like a true researcher - he had data for everything he said and was very careful and hesitant about jumping into conclusions unlilike others.
He introduced his lecture by quoting the size principle and how the Type 2 fibers, which has the greatest potential for muscle growth, gets recruited at the end of a set. Then he talked about the infamous Dr. Phillips study which showed how low load, high volume protocol (30RM) showed greater protein synthesis compared to a high load, low volume (90% RM) protocol. He also showed another study by Wilborn et al., ( 2009) which showed molecular markers and proteins for muscle growth all increased significantly for both 18-20 reps and 8-10 reps. Both these studies lend some credence to the fact that high reps may be valuable for increasing muscle growth.
But, mind you, both these studies are acute studies in beginners and measure surrogate measures not muscle growth. Chad also mentions this and how we have to be careful since this an acute design. I asked him about how this could be muscle-specific since both the studies were done on leg musculature and we have heard plenty of stories about 20 rep squats and how people grow better with high reps for legs.
The second half of the presentation was by Dr. Coil Wilborn about training to failure which I will cover in the next part.
It is very important to draw lines between what we know, what we do not know and what we need to know. Unlike what most people think, things aren’t as black and white and are mostly shades of grey. Anyway, that’s all I have for the first part.
Related Articles

How To Read a Study - The Pyramid of Outcomes
July 16 2011
The outcome measured in a study is the most important aspect of a study. But this aspect is the least emphasized when people try to interpret studies. So which outcomes are the most beneficial according to the pyramid?
What does the pyramid say?
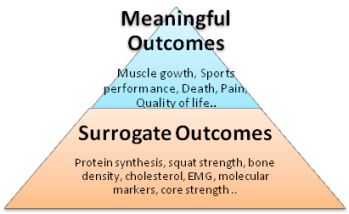
Base of the pyramid: The base of the pyramid include studies with outcomes which do not have a direct impact on you. These are called surrogate outcomes. Examples for surrogate measures are protein synthesis, EMG analysis, X-rays, in-vitro models, cholesterol and so forth.
These measures are ‘stand in’ or represent meaningful outcomes higher up in the pyramid. For example, we think that protein synthesis is a stand in for muscle growth. We think x-ray is a stand in for pain outcomes. We think cholesterol levels are a stand in for deaths due to heart disease.
Top of the pyramid: As we go up the pyramid, we get to the patient or meaningful outcomes which are the most important and has a direct effect on you. Examples of these are muscle strength, muscle growth, fat loss, death, pain and so forth.
As we go up the pyramid, the importance of the study and the outcome goes up too.
What about some examples about surrogate measures?
Muscle growth: The most popular surrogate measure for muscle growth is protein synthesis. What people care about is muscle growth. We are not really sure if an increase in protein synthesis will lead to an increase in muscle growth. It may - or it may not. The molecular makers like AKT, MAPK, mTOR are surrogate measures for muscle growth which are way below the pyramid.
Even if synthesis goes up, protein breakdown could go up too. Or the fatigue generated can go up and cause the person to lower the weights or reduce their training. All these can affect muscle growth in a negative manner.
Performance: One of the usual performance measures for an athlete is the increase in squat strength. But can the increase in squats increase how many goals you scored, decrease the time taken to run or make you throw or hit longer? There are a host of factors that can influence performance, and squat strength may or may not be one among them.
Bone density: Bone density is a classic example of surrogate measure. We do not care about bone density. What people care about is does it lower the chance of a hip fracture, the most disabling kind of fracture.
People could fall due to poor vision, lack of strength, balance, their environment and so forth. So an increase in bone density may not always translate to fewer fractures.
Cholesterol: Drug companies usually measure cholesterol levels to show the efficacy of a certain drug. But the question is do they make the person live longer or do they feel better?
Clofibrate, a drug for cholesterol, lowered cholesterol really well, but inexplicably increased the number of deaths. A recent example is the popular diabetic drug -Avandia - for lowering blood glucose. The drug worked really well for lowering glucose levels in diabetes, but people suffered from heart attacks, stroke and even deaths. These are good examples of drugs that got approved from surrogate end point studies.
Core strength: In the fitness field, there are lot of people who quote studies showing increase in EMG, core strength, pig spine models, shear /compressive stress values as evidence for prescribing or not prescribing certain exercises for the core. These are just surrogate end points. Until they can show the intervention can increase performance or prevent injury or decrease low back pain, it is just a beautiful hypothesis.
Exceptions: There are cases where just lowering the symptoms might be really important for you. For example, people in end-stage cancer treatments, improving the quality of life or the symptoms can be very important. There are also surrogate measures which are highly correlated with the end point.
Why do people use surrogate measures?
Practical Application
Related Articles

Should I Take a Wide Grip or Close Grip for Lat Pulldowns?
July 02 2011
This is the most common question I get asked when I talk about lat pull downs to a new client. As you will see, this question also gets to the root of one of the major problems.
Does changing grip width make a difference?

The Magnitude of Effect: In research, they call this the “magnitude of the effect”. If you change your grip from narrow to wide grip, how big of a difference will it make on your physique? Good researchers worry about the clinical significance than just statistical significance.
Even if you do all the adjustments with the grip, 90% of the people who come to the gym will never come to that single digit body fat level where they could tell these small difference in lats. They should focus or worry about things which will make the biggest difference.
Population: If you are a bodybuilder, you are justified worrying about the grip width and such. You will be getting down to 4-6% body fat levels where the judges can clearly see how well your lats look in the lat spread pose.
This is one reason why wise men say never copy routines of bodybuilders. Their goals are way different from the majority of the population and their training will reflect them. Their priorities are a lot different than yours. This also one reason why ‘some’ bodybuilders do not make the greatest of trainers.
Other examples: Some other examples where people worry about the minutiae and forget the big picture are:
1. Spending hours doing cardio but have no clue about their food and calorie intake
2.Doing high reps to burn more calories or /and trying to burn calories using weights
3.Focusing on isolation exercises like curls & shoulder raises
4.Doing half an hour of ab exercises
5.Eating a ton of protein , but not getting enough calories in the first place.
I will stop here, but I can just keep going.
So what should I focus on?
Three things: The three most important aspects which will make the biggest difference in your physique are your diet, weight progression, and sleep.
Just pull: As long as you are pulling and getting stronger, you are doing it right. It doesn’t really matter if you are doing lat pulldowns or chin ups, close grip or narrow grip or whatever.
If you are good with the first 3 points, then you are welcome to worry about little things like how many reps, which grip, and so forth.
But does the grip width make a difference?
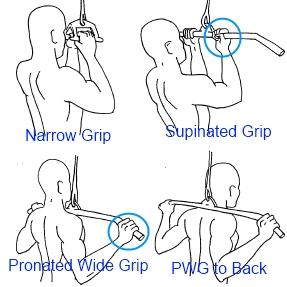
Practical Applications
Related Articles
The Fall of the Greatest Theory of Muscle Growth - Part 2
May 22 2011
If you haven’t read the first part of the article and is not aware of the debate, please read the The Fall of the Greatest Theory of Muscle Growth. Recently, another study was conducted by a different group of authors and concluded that the acute hormone elevations may help. Now let’s take a closer look at the study titled:Physiological elevation of endogenous hormones results in superior strength training adaptation.

What was the design of the study?
The same design was employed in the previous study too, but the big difference was that the leg exercises were performed after the arm exercises But in the current study the leg exercises were performed before the arm exercises.
What were the results of the study?
My Comments
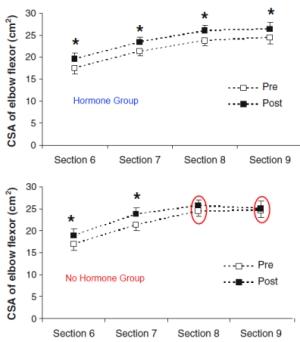
Practical Applications
Related Articles
Pain Is In Your Brain
May 18 2011
You will only feel pain if the brain thinks that the stimuli is threatening or it is a danger to the body. And this is what I tried to convey in my pain article. Check it out if you haven’t read it. But most people can’t fathom this concept.
In the below presentation by Lorimer Moseley – one of the leading researchers of pain- he talks about the concept of how ‘pain is in the brain’ by giving an example from his own life. The post below talks about this example.
Scenario 1
Scratch from a twig: This was 8 years ago when Moseley was camping in western Australia: Something touches the left side of his leg when he is walking on the trail through the woods. It activates the nociceptors (pain receptors)
Brain thinks: This is not dangerous, we have been here a million times, I grew up walking bare foot in a bush. My nick name was scratchy because I used to have to so many scratches on my leg. So the brain says kick of the twig and get back to business. (Remember this evaluation by the brain is outside of your control or awareness. It happens in a split second)
No Pain: Here he feels no pain since the brain do not think it is threatening and you need to be protected.
Result: 3 days later he wakes up in the hospital. He was the first survivor of eastern brown snake (grade 3 bite). The bite works by stimulating the nerves and hence it ‘should’ be extremely painful.
Scenario 2 (6 months later)
Scratch from a twig: 6 months later he was walking down the bush and something scratches the left side of his leg. It activates the nociceptors (pain receptors) as usual.
Brain thinks: This is highly threatening since last time I was in the bush and a twig scratched, I almost died. So this scenario is really threatening and he needs to be protected. (Again, evaluation by the brain is outside of your control or awareness. It happens in a split second)
Extreme Pain: There is extreme pain and he falls down and is holding his leg.
Result: It was just a scratch from a twig and ‘should not’ be painful.
The stimuli is the same in both scenarios. One is extremely painful and the other is not at all painful. What changed? The only thing that changed is how the brain perceives the stimuli, and it really doesn’t matter if the pain receptors are activated or not!
Conclusion
Related Articles
The Biggest Loser Show Review
May 14 2011
Since I work in a fitness center, I hear a lot of people talking about how the Biggest Loser contestants can lose so much weight and how they wish they could lose the same or if they had a celebrity trainer. Let us take a closer look at the Biggest Loser show.
What is the biggest loser show?

TV Show: Biggest Loser is a weight-loss contest aired on NBC which has become extremely popular. It is broadcast in different countries with each having their own versions. But the central theme in every show is all about who can lose the most weight in 12 weeks for a cash prize. Contestants lose 100-220 lbs in 12 weeks.
What are the pros of the Biggest Loser show?
Entertaining: The show is entertaining to say the least. The ratings of the show are proof that they got something right about the show.
Inspirational: It is inspirational to see people making an effort and achieving their goals. The message of “If they can do it, I should be able to do it too” is clearly infectious.
What are the cons of the Biggest Loser show?
Unrealistic: The show is completely unrealistic. Most people cannot achieve that sort of weight loss in such a short span of a time (and shouldn’t). You can though if you have the following going for you:
Weight Maintenance: I have written in the past that losing weight is easy, maintaining it is the hardest. You have to do everything (and more) that you did to lose weight for the rest of your life to maintain the new weight.
The faster you lose and the more you lose, the harder it will be to maintain that weight loss. The Biggest Loser contestants lose around 50-60% of their weight in 12 weeks which is 10-15 lbs per week. The recommended guidelines suggest 5-10% of your body weight at 1-2 lb weight loss per week! How is that for ‘following’ guidelines?
And this is one major reason why most of the contestants gain most of their weight right back after the show. They are now their back to real life where they have jobs, a family to take care, responsibilities, and so forth. And worse yet, for some -along with the weight gain- comes the psychological problems of defeat and failure which triggers a vicious cycle of overeating, depression and guilt.
On the other hand, most contestants who are maintaining most of their weight have turned their life completely upside down. These people have become fitness experts for a career and they advise and coach people in losing weight and staying healthy. This sort of drastic life change is unrealistic for most of us.
Extreme Workouts: People who weigh 300-400lbs who even have trouble walking and are at high risk for cardiovascular problems are made to run for miles which is outright dangerous and ridiculous.
Some of the technique they use in the weight room are just good examples of how NOT to do those exercises. Contestants are made to do cardio for hours a day which is above and beyond over-training and is a great way to have long lasting knee and ankle problems. The concept of intelligent workout programming is missing; it is all about throwing as much stress as you can to the body.
Extreme Water Loss: Some of the contestants in the show have dropped 20-35 lbs in days by dehydrating themselves using extreme measures like working out in rubber suit and not drinking water for 24 hours and such. This isn’t actual weight loss and can mislead people who are unaware of these extremes measures
Practical Considerations
Related Articles

The ‘Train Low, Compete High’ Protocol for Endurance Training
April 30 2011
Train low: Train low means to perform your training under low glycogen levels.
Compete High: Means competing under high glycogen levels.

Why do you need glycogen?
Energy : Carbohydrates you eat are broken down into glucose and stored in your muscles as muscle ( and liver) as glycogen. Glycogen is your primary energy source for endurance events like long distance running and such.
Sports nutrition guidelines: Hence current sports nutrition guidelines recommend a high carbohydrate intake for endurance training. This is called the “train high, compete high” approach.
So why train with low glycogen?
If glycogen is required for energy, why train at low glycogen levels? This goes against the conventional training wisdom, right?
Cellular Signal Pathways: The recent discovery of the several molecular pathways activated during endurance training (AMPK, P38, MAPK and so on shown in the figure) shows that these signaling protein are activated to a greater extent when exercising with low muscle glycogen than normal or high glycogen levels. These pathways play a critical role in making new mitochondria and activating other training adaptations.

2005 Study: The 2005 study by Hansen confirmed these suspicions. In this study, seven untrained males undertook a 10-week program of leg knee extensor ‘‘kicking’’ exercise. Interestingly, the study showed a “two fold” increase in time to fatigue in the Low glycogen leg compared to the high glycogen leg which goes completely against the current training philosophy.
The study seems to show that it might be the lack of substrates (glycogen) and not the surplus of substrates which activates the endurance training adaptations.
What about training and performance measures?
But the question is will this concept of Train low, compete high work for trained individuals and translate to increased performance?
Studies: Number of studies was conducted to see if there is an improved performance with low glycogen training. Guess what, none of the studies saw any increase in performance measures besides the increase in these signaling pathways.
This is another classic example of how it is so important to test our hypothesis with meaningful outcomes before jumping to any conclusions, not matter how sensible and beautiful the hypothesis may be.
So why didn’t we see any performance improvements?
Practical Consideration
Related Articles
Scans for Low Back Pain: Good or Bad
April 19 2011
This was a really interesting post by Neil O’Connell at bodyinmind.org.This is such a relevant post because almost all of us will have some sort of low back pain in our life.
We now clearly know that abnormal findings on the x-ray and MRI ( like disc herniations, bulging disk, degenerating joints and so on) are clearly NOT related to the onset, severity, prognosis, or duration of low back pain.

This is now so well established that the American College of Physicians have come forward with clinical guidelines saying” Clinicians should not routinely obtain imaging or other diagnostic tests in patients with nonspecific low back pain”
Non-Specific low back pain is defined as low back pain that cannot reliably be attributed to a specific disease or spinal abnormality. 85% of the low back pain is due to non specific effects.
Imaging is only recommended for a minority of people whose low back pain can be attributed to specific pathology like cancer, compression fracture, spinal infection, cauda equina syndrome. progressive n neurological deficits and such.
Though these guidelines exist, physicians routinely get scans for patients. But the question is there any harm? The answer is YES.
I am not going though the design specifics of the study. You can check the link for more info.
This post again emphasizes the powerful role of the psycho-social factors in pain which are still missing in our thinking about pain.
The Llnk to the post: http://bodyinmind.org/spinal-mri-and-back-pain/
Related Articles
NSCA Personal Trainer’s Conference 2011 Part 2
April 17 2011
This is the second part of the Review. If you want to read the first part, click here.
Chad Kerksick
Dr. Kerksick is an Assistant professor at the University of Oklahoma in the Health & Physical Education Department. Chad’s Title of the presentation was “Split Training”: A training approach to effectively teach, train and monitor clients”.

Chad was the typical researcher- he had references for everything he said and his slides were just replete with studies. And he spoke with a dry and unemotional tone like a true researcher. He gave an outline about the various resistance training variables like loading, frequency and such and then talked about split routine. His split routine was the typical 2 days lower, 2 days upper body.
The summary was that split routine is an efficient training model since we can use higher volumes, there is more recovery time and it allows people to train at the recommended frequency and intensity. I was waiting for a study ( or studies) which showed greater increase in strength or muscle with a split body routine compared to a full body routine. But he didn’t have one. If the adaptations are similar , why spend one more day in the gym when you can spend 3 days and get the same benefits? I just felt like he didn’t have a compelling conclusion to why someone should do a split routine.
In one of the slides, he showed a study done by Kramer and how it increased serving velocity and jump height by 13 percent, but the results weren’t statistically significant. He talked about how 13% increase is clinically significant thought it may not be statistically significant. This is one of the concepts many people are unaware of. Mark Young, one of my smart friends, talks about his concept in his new “How To Read Fitness Research Product”. If we are using p values, we should do a power analysis to find the minimum samples we need to have a clinically significant result to be statistically significant. This is especially important in the exercise field when we are dealing with very few sample sizes. Unfortunately, not many exercise studies bother to do one.
I asked about power analysis and confidence intervals after the presentation. I also asked him why he thinks in most studies there is a plateau of strength by the 4th or 5th week. He said he has seen the same in his studies too. I also asked him about his view about training to failure. He said he ‘believes’ in going to failure in atleast one your sets. I was looking for a more scientific answer though or any relevant studies. He also talked about the hormone hypothesis which I still think is just an interesting hypothesis lacking causative studies.
Brad Schoenfeld
Brad is the Associate Editor of the NSCA Strength and Conditioning Journal, an adjunct professor of exercise science, manages a fitness corporation, has a blog (www.workout911.com), and has written a few books. Brad’s presentation title wasThe Functional Fitness Continuum: Training Strategies to Optimize Functional Transfer. Brad lectured for a half an hour and Jay Dawes lead the hands-on session.
This was one of the best presentations at the conference. It is a very relevant topic which is still misunderstood and misinformed even among fitness professionals all over the world. There is rage in the fitness industry to make everything functional these days
People usually say machines are non-functional and hence they have no purpose. Brad showed a study which showed older individuals who used ‘leg extension machine’ to improve their walking and balance considerably. In fact, 2 of the subjects were able to walk without the assistance of the canes. He also showed how free weight training increased functional strength more than machine training. In short, all modalities can elicit functional improvements, and the greatest transfer is seen with free weights.
His next point was unstable training. You will be hard pressed to find a gym where people don’t use bosu balls or unstable surface training. Atleast, I get to see it 60 hours a week! Most of our movements are done on a stable ground so training on an unstable surface is ‘non-functional’. The more unstable the movements lower the loading on the muscles. And lower the loading on muscles, the less the increase in strength, muscle and such. The funny thing was last year in the same conference there was an hour and a half presentation on unstable training. I asked him if there is any benefit of unstable training on propioreception when you are recovering from an injury.
He talked about how single joint exercises are considered non- functional , but can fill the ‘gaps’. For example, only 50% of the hamstrings are involved in squats compared to glutes and quads. Brad also emphasized the importance of fast repetitions in functional training since movements are velocity specific.
I talked with Brad a couple of times during the conference. At the end of the conference, we went and had dinner. We talked a lot about research and the problems in the fitness field. I was really excited to talk to someone who is very knowledgeable in both research and application. I usually don’t get people of this caliber to talk shop and hence speaking with Brad was one of my conference highlights. You will see a lot of people who are evidence-based and such, but there is only a handful of people who are really concerned about the profession and wants to bring some credibility to the field of fitness. Brad is one among them and I felt like we both had a lot of things in common.
There were a few others good ones too. One was by Lee Brown about Speed Training. Lee is an excellent presenter and really brought down the topic so that everyone could understand. Some of the presentations I felt were a bit too heavy on physiology and lacked on the application aspect. Maybe it was the way they presented since most of them were researchers. I also made it a point to network with a lot of trainers at the conference.
Anyway, that’s the end of the review.
Related Articles
NSCA Personal Trainer’s Conference 2011
April 09 2011
The conference was held in Las Vegas as usual. I had reviewed the 2010 conference here. It was a 2 day conference and each presentation lasted around an hour and a half. They had both hands-on and lecture type presentations.
Marie Spano MS
She is one of the leading sports nutritionists and co-authored the book ‘NSCA’s Guide to Sports Nutrition’. The title of her presentation was “Analyzing the popular weight loss diets”.
This was a really good presentation. She reviewed popular diets, what is good and bad about these popular diets, really emphasized how important it is to make behavioral changes than focus on diets, avoiding the diet mentality, and so forth. She talked a lot about intuitive eating and how it is a great way of avoiding the diet mentality and the popular food and eating ‘rules’. Everything she said was all about long term adherence, proper nutrition, and a healthy mentality towards food, your body, and eating. And everything you see and hear around you is the exact opposite: quick fixes, no mention about nutrition, and rules like ‘eat this and not that’.
Below are her food rules:
1. Incorporating high volume foods
2. Drinking water before your meals
3. Eat half your plate with fruits/veggies
4. Eat 20 gms of protein with every meal
5. Tune into physiological hunger
6. Eat when you are hungry
7. Work on emotional eating
8. Find out why you eat
9. No food, within reason, is off limits.
10. Learn to like healthy foods,
11. Create what fits into your lifestyle
12. Change your environment
13. No good food, bad food
14. If you bite it, write it
I asked her if she emphasizes fat loss with her clients, how much nutrition you can talk to your clients, and about re-feeding. I just felt she could have mentioned about the “starvation mode” or metabolic drop seen in people with dieting, strategies like re-feeding or cheat meals a bit, and what is wrong with the popular ‘The Biggest Loser’ show.
Most of our diet advice comes from diet experts who work with bodybuilders and fitness models who need to come down to single digit body fat levels for a few weeks or months. We try to take their advice and apply it to the general population who doesn’t have even half the motivation of a bodybuilder, nor the genetics, they need to look good the whole year, and don’t need to come to insane body fat levels. And that’s the problem.
Just so that you know, it is hard to make all these changes in people’s lives though this maybe the right way. I guess the question is how to make these behavioral changes, will these really help lose weight and keep it off and such. So it is not as black and white.
Dr. Len Kravtiz
Len Kravitz, PhD is the Program Coordinator of Exercise Science and researcher at the University of Mexico.
Len did a presentation on Eccentric Training titled” Eccentric Training: Everything you wanted to know and more”. I don’t think I have seen many presenters who are so enthusiastic and animated. He is one of the rare breed of teachers who can spark the love for the subject in a student.
He spent around 30 minutes on the physiology of eccentric contraction which I thought was a bit too deep for the audience. He talked about titin, troponin and such, and trainers don’t care about that stuff. But he presented the subject better than anyone I have seen. I remember him walking around the room and animatedly saying, “you become the actin” and talked about how he makes his students act out the muscle contraction. I wish more teachers could watch him.
His presentation was mostly about the mechanisms, theories and lacked a bit on practical-based information I felt. He showed a study about how eccentric contractions increased concentric strength. But this was just an acute study and did not say much about long term adaptations. It is clear that eccentric training increases concentric strength, but concentric contraction are better than eccentric contractions to increase concentric strength in the long term. It is just the specificity principle in action.
This is the reason why we should look at systematic reviews and meta analysis first. If we don’t have any, then we fall back to single studies. I had written an article about eccentric contraction based on a meta-analysis here. I am surprised how he missed that met-analysis. I also felt he could have talked about how eccentric contraction show increased muscle growth than concentric contraction which is one of the most talked about benefit and the reason why most people use it. He showed a study which showed eccentric contractions burned 8-9% calories post-workout for many hours. And 8-9% is how many calories I was thinking? 10, 25, 50?.
He showed a lot of videos about how to do eccentric contractions. I think two or three would have been fine to show the different ways to overload. He had too many I thought, and people didn’t like the kid in the video who was bent on showing the world how strong and awesome he is. I talked to Dr. Len and even had lunch with him. He seems to be a real nice guy and is very humble and polite.
Conclusion
This is getting too long and I will write more about other speakers in the second part. I felt the presentations were a lot more evidence-based than last year and they made an effort to pick speakers who have PhD’s and do specific work in that particular topic. I just wished they had more topics about training and nutrition for muscle growth.
That’s all I have for Part 1
Related Articles
A Revolution in the Understanding of Pain and Treatment of Pain
March 29 2011
This is an article I wrote for another website. This is will change the way you look at your pain forever.
Click the below link to go to the article please.
A Revolution in the Understanding of Pain and Treatment of Pain
Related Articles
Detox Diets and Cleansing Diets: Do They Work?
March 14 2011
What are detox diets and cleansing diets? Do they really get rid of toxins and chemicals from your body? And do we need to cleanse ourselves every now and then?
What are detox diets and cleansing diets?
Basic Premise: The basic premise of every detox and cleansing diet is that our body is constantly accumulating toxins and chemicals from the food and our environment . And we need to get rid of these toxins every now and then.
Duration: These diets last for a short period of time, usually 4-8 weeks.

Methods: Some of the common methods include one or more of: dieting, using herbs and supplements, consumption of specific foods such as fruits and vegetables, juices or water or avoiding fats, sugars, fasting, avoiding caffeine, aclohol, junk food and so on. Some others involve extreme measures such as colon cleansing, liver flushing, chelation, and so on.
What do these diets claim?
Toxin Removal: They claim that these diets or therapies can effectively remove toxins or chemicals trapped in the body through urine or bowel movements .
Benefits: By removing these toxins, they claim that you will have improved energy, clearer and fairer skin, a regular bowel movement, improved metabolism and digestion, increased concentration, and will also prevent diseases.
Now can these diets really remove toxins?
Scientific evidence: There is no scientific evidence to show that you can remove toxins or chemicals using these methods. Chelation, a medically approved procedure, is used to remove heavy metal toxins when people suffer from genuine iron, lead, uranium poisoning. This is only warranted when the levels are dangerously higher than normal.

Pictures: There are pictures on the web of these long algae like substance from bowel movements called mucoid plaque. These are not toxins or chemicals, but they are formed from bentonite and psyllium husk which are most often included in colon cleansers. The bentonite acts like a clay to expand when it mixes with water. The psyllium husk adds bulk and are used as a source of dietary fiber. They are the “toxins” from the very substance which are supposed to clear the toxins.
Foot pads: These foot pads, left on your feet overnight, turns brown in the morning. These pads have powdered wood vinegar which turns brown when it comes in contact with sweat. These pads also peel off the dead cells on your feet which gives them the brown color. It’s funny how toxins are always brown in color and not green or blue.
But what about these chemicals accumulating in the body?
Chemical-Free Life: You cannot lead a chemical-free life because everything is made of chemicals. For example: an average person has more than a trillion atoms of uranium in their body and that hundreds of these atoms are radioactively disintegrating every day. All is coming from a perfectly natural source: the food we eat! Many toxic substances occur naturally in foods, e.g., arsenic, but in doses so small to even bother about.
Dose: The toxicity of a chemical depends on the dosage or the amount received. Aspirin - a wonder drug- in extreme doses becomes toxic and causes acute renal failure, coma, and heart failure. Botox ,one of the most toxic substance know to man, is safely used in cosmetics because it can be highly localized. There is no chemical that can be automatically labeled as dangerous or safe without the above info.
Body’s Detox:Our body has its own detox like the gut which prevents entry of toxins, the liver which breakdown harmful chemicals which are then excreted by the kidneys. None of the above processes can be made more efficient by detox or cleansing.
But what about people feeling better?
Increased Energy: This boost in energy is due to fasting. This is one of the body’s survival mechanism to get you moving to locate food during starvation periods.
Weight Loss: If you are on juice and water and other low calorie diets, you will lose weight. Don’t worry, this is just temporary and you will put all of it right back on when you go back to your regular diet.
Feeling Better: You will feel better if you stop using alcohol, caffeine, junk food, stop smoking and such. That is just common wisdom, right.
Other Benefits: The other benefits like clear skin, improved digestion, increased concentration can be easily traced backed to increased water intake, fruits and vegetables, avoiding too much fatty foods and such.
Placebo effect: If you really believe something is good for you and is helping, you will feel it too even if has nothing medicinal in it. Check this short video about placebo effect.
The bottom line is whatever you are feeling on a detox diet or cleansing diet has nothing to do with removing toxins.
Practical Applications
Related Articles

What is Autoregulatory Training?
March 09 2011
What is autoregulatory training? Is it the same as instinctive training and how can you apply it?
What is autoregulatory training?
Autoregulatory training: It is a training method which makes sure that you are using the maximum weight for a particular repetition, say 6 repetition or 10 repetition.

Why the heck we need autoregulatory training?
Planned Training: Planned training may not be familiar to bodybuilders or the common folks. But it is pretty much the norm for athletes to plan their workouts months and months ahead. This includes the weight they should use, number of days they train, the reps and sets. It is called Periodization.
Problem: The problem with this planned training is an athlete due to so many outside variables like sleep, food, stress and such may either find the weights too easy or too hard on a particular day than what was planned months ahead.
Solution: One solution is to use weights based on how much you can lift that particular day than what was planned. And this weight also gives you the starting weight for the next workout. This is basically called autoregulation training.
What about instinctive training?
Instinctive training: In instinctive training, you use a weight depending on how you feel that day. You do not test a weight like autoregulatory training from last week to change your weights accordingly. For example, you didn’t sleep well last night and feel a bit tired and hence you pick a weight which is a bit lower than your last workout.
In autoregulatory training, you lift the weight you did last workout, AND then change the weights for the next sets based on how many reps you got with that weight. Some folks can tell how they feel from their bar speed and how they feel in their warm up sets
Are there any studies on autoregulaton?
There were 2 studies done on autoregulation comparing it a regular linear periodization.
15 week Study: There was a 15 weeks study done on untrained females back in 1996 which showed no significant difference in strength between periodization and autoregulation. In fact, the periodization showed a linear increase throughout the study while the autoregulation group showed a plateau at the later stages of the study.
6 week Study: This was a recent 2010 study done on Division 1 football players which is quoted everywhere as an example of autoregulation. The study has numerous limitations as shown below:
The study is interesting, but only brings in a hypothesis which needs to be tested with a well designed, randomized-controlled study.
Practical Application
Related Articles
No Arms, No Legs? No Worries
March 05 2011
If you think you are weak, fat, skinny, ugly, unfortunate, and all the negative things you can think about you and your life, this short video is for you.
This is part of the series of inspirational videos I am putting together under the category “Inspirational”. If you come across any more like these, please send it to me.
Related Articles
How To Make Fitness Goals and Achieve Them
March 01 2011

Use this simple step by step approach to make and achieve fitness goals.
Please click here to read about making fitness goals
Related Articles
What is the Placebo Effect?
February 23 2011
We all heard about the placebo effect. Here is a nice little video explaining what it is and what it can do for you.
Related Articles
Does Nitric Oxide (NO) Supplements work?
February 08 2011
Nitric Oxide (NO) supplements are one of the most popular pre-workout supplements. NO explode is one of the top selling pre-workout supplements at bodybuilding.com.
The major claim of nitric oxide supplements is that it increases blood flow the muscle and can bring in more oxygen and amino acids. ( and thereby increase muscle growth). But is it true?

What is Nitric Oxide?
Why is nitric oxide such a popular supplement?
But Can nitric oxide supplements increase blood flow?
Can nitric oxide supplements increase protein synthesis with resistance training?
Practical Application
Related Articles
Does the Shake Weight Work?
January 31 2011
Shake Weight is the new fitness product which is the talking point these days. Of course, the guy and the girl who uses it is ripped. So it should work. Or does shake weight work? Here is my shake weight reviews.
What are the Shake Weight claims?

1. Get toned & firm arms in 6 minutes a day - for women.
2. Build definition, strength & size in 6 minutes a day - for Men.
So does the Shake Weight work?
Since there is no shake weight study out there, all we need to see is if shake weight goes against the fundamental science of muscle growth and fat loss.
Are there any risks with Shake Weight?
Practical Applications
Related Articles
Functional Movement Screen: Is it Really a Screen?
January 21 2011
FMS is a battery of 7 movement tests which claims to predict injuries and even prevent injuries. It is becoming very popular among NFL players and other fitness professionals.

From what I have seen, the majority of people who use the screen are personal trainers. I wrote a review about FMS when I attended a 2-day seminar 3 years back here (Functional Movement screen).
Gray Cook, one of the brightest and most eloquent in the industry, in one of his recent podcasts talks about how FMS screen should be used on everyone just like a blood pressure screen. Let us see if FMS can be used as a screen or not.
What is the difference between a diagnosis test and screen?
Diagnosis: People are sick and they “come to you” because they want you to diagonoze why they are sick.
Screening: People are well and healthy and might be coming to you for some unrelated problems, and we are “soliciting them” telling that they will live longer or live better if they let you test them.
So what is the problem with FMS as a screen?
Screen Requirements: When you employ any type of screen, the validity of the screen should be of the highest quality since you are “labeling” people.And hence we should have some very solid proof that people will be better off in the long run. When someone scores less than the cut-off score in the FMS, you tell them that your chance of getting injured is extremely high. This is a great way to get someone move less or have fear of movement or spent their time and money trying to fix it with their trainer.
Injury Prediction: FMS has not been tested on the lay people, and hence we really don’t know if people will get injured if they scored less than the cut-off.
Injury Prevention:If they proved that FMS can indeed predict injury, then they will also have to prove that if you were to fix the movements that it will reduce the chance of getting injured. And FMS has not been shown to prevent injuries. If you can identify injuries but can’t prevent injuries, then you better not label people or screen them in the first place.
Frequency & Severity: The importance of any screen will depend on the frequency and the severity of the problem. When FMS is used on lay people, you have to ask what is the severity and frequency of injuries. In NFL FMS study, 13 people out of 46 got injured in 4.5 months (28 in 100). For the lay people, we might get 1-5 injuries out of 100 people in 1-3 years!
False positives & negatives: Every screen or test has false positiives & negatives since no test is 100% accurate. For example, even mammography screening will falsely diagnose of someone having breast cancer, when they don’t have it or falsely diagnose of someone not having breast cancer when someone has the disease. The measure of these are called the sensitivity & specificity of a test
In the FMS study for NFL players, the sensitivity was 46%. That means out of 100 people who will get injured, the test only identified 46 of them correctly, which is less for a screening test. A screening test needs high sensitivity (90%) because we want to identify as many people with the disease because we think this disease is of such importance that people need to be screened for.
Cost Vs Benefit: If we finally “prove that FMS indeed predicts injuries and prevents”, what is the cost vs benefits here? Imagine your client comes to get in shape as most lay people do. You do the FMS, finds dysfunctions, and tell them that their likelihood of getting injured is high. Though that wasn’t their goal or priority, you make them go through the FMS screen fixers for 10-15 minutes for which they have to pay 50-100 dollars an hour.
So you have to ask yourself, with any screen, does all this time, money, and anxiety people have to go through, will it improve the quality of life in anyway? Will trying to minimize an injury which has the chances of next to nil in years improve her quality of life? Probably not.
But what about an NFL player? For the NFL players, the benefits are huge. The severity and frequency of the problem is so high, the risk of getting injured is next to losing millions and their career. FMS also shown to predict injuries in NFL in one study. Injury prevention should be their primary goal.
Other: FMS is available, affordable & not that time consuming which is indeed a plus for any screen.
Practical Applications
Related Articles
What are your chances of getting cancer?
January 09 2011
Cancer and other cardiovascular diseases are pretty common these days . Usually the chance/risk of you getting /preventing/ treating cancer/other diseases is usually expressed in percentages since we are not certain about their outcome.

But sometimes these percentages can be deceiving.
Which drug will you take to lower the risk of cancer?
Which drug will you take? Obviously, Drug A.
In fact, it doesn’t matter which drug you take: The risk reduction of 25% and 0.1% ,though looks different, is in fact the the same for both the drugs
How can Drug A & B have the same effect ??
It is because the percentages are just expressed differently as in absolute vs relative risk. Risk or chances of you getting/preventing/treating a disease is usually expressed in absolute or relative risk. The risk always appear bigger when expressed in relative risk than absolute risk as you can see.
For example, consider 1000 women who did not take the drug A/ B and another who did take. Within 10 years, 4 die in the first group an 3 in the second group which did take the drug of cancer as shown in the picture. You can see how we got the absolute and relative risk reduction.
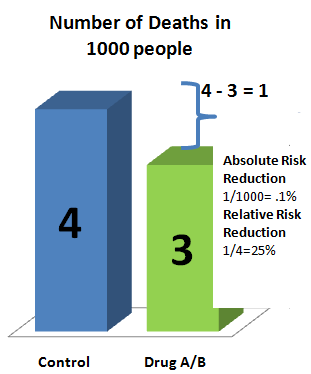
How do people use this information?
Practical Application
Related Articles
Does It Work?
January 01 2011
Being in the fitness field, the usual questions I get are Does it work? Does P90X or crossfit works? I heard it works, Is it good for you? and so on.
But these question lack three important parts to make it meaningful:

Works for what?: It means is it for strength, muscle growth, fat loss, flexibilty, cardiovascular endurance and so forth. The “what” is important because to optimize each of these goals require a different training or workout program.
For example, crossfit will work for strength endurance since it involves a lot of high rep training, but won’t be the best for maximal strength. Yoga works for flexibility but not good for strength muscle growth, or cardiovascular health. Running works for fat loss but not for building muscle.
Works for who? You have to specify the population you are trying to use it too. The who is important because results can be completely different based on your training level, age, gender and so forth.
The whom depends on the type of question. For injury prevention, the age, the gender, sport played, and the level can have different effects on injury prevention. For example, females have 4-8 times ACL injury than males, soccer will have more ACL injuries than cycling. A training program to increase strength and muscle for a beginner won’t work for trained individuals. A drug which works for men may not have the same effect on females too.

Compared to what? When you say the program X it works, what are you comparing it to?
For example, when you say P90 works, are you saying P90 will increase strength and muscle more than not working out? Of course, it will. Or are you saying P90 works better than a general 3 sets strength and cardio routine? Maybe. If you are saying P90works for increasing maximal strength than a powerlifting routine. I will say of course not.
In drug studies, the comparison group gets a placebo ( a drug which has no effect but it looks, smells and feels the same). The goals of the drug study is to see if the new drug works better than the placebo drug. So the placebo works too, but compared to a real drug, the effects are not great.
Practical Application
Related Articles
Is Muscle Soreness A Reliable Indicator of Muscle Growth?
December 28 2010
Is muscle soreness a reliable indicator of muscle growth? Most people think it is. If they get sore, they think they had a great workout and in turn will grow muscle. If they don’t get sore, they feel they didn’t do enough to cause muscle growth.
What is muscle soreness?

Discomfort or pain in the muscle caused by unfamiliar physical activity. It shows within the first day and peaks within 2 days, and then disappears within 5-7 days. Hence it is called DOMS or Delayed onset of Muscle Soreness.
What causes muscle soreness?
There are so many theories proposed, but none has conclusively be proven to cause soreness. The current theory tries to explain soreness through a combination of theories.
1. Muscle and connective tissue damage due to high forces, especially eccentric contractions (means lowering the weight).
2. Increased ca leakage from the muscle and inflammations worsen the damage
3. Sensitizes and activates the pain receptors to cause pain and discomfort.
So why Is muscle soreness NOT indicative of muscle growth?
Muscle damage not required: Muscle can grow with just tension and no damage. Most people think that damage is required for muscle growth.
Receptors called integrins can sense mechanical load and activate pathways which are required for protein synthesis and thereby muscle growth (Integrin Mediated signaling). So even if you are not sore, you might be very well growing.
Soreness not indicative of the level of damage: You could have done the same muscle damage, but the pain receptors get less and less sensitive with damage . So you don’t feel the soreness, though the damage is still present and maybe even more than when you had soreness. So soreness is not a reliable indicator of the magnitude of muscle damage either.
More soreness do not mean more growth: It doesn’t matter how hard you hit the muscle or how many sets you do, the protein synthesis levels can only go up so far. So more soreness do not mean more damage and more protein synthesis and hence more growth
More Soreness may mean less muscle growth: Unlike synthesis, protein breakdown on the other hand, will go up with greater damage. So when you are really sore, it could also mean that you are breaking down more muscle and in turn growing less!
No soreness results in muscle growth: People have experienced muscle growth without soreness. Low reps hardly ever cause soreness, but powerlifters who does low reps all the time are as big as bodybuilders.
Major soreness results in little muscle growth: People get really sore from endurance training like cycling and running or playing ping pong. But they don’t grow any appreciable muscle compared to lifting.
Practical Applications
Related Articles
Carbs Not Required for Your Workout Protein Shake
December 20 2010
The belief that carbs are required in your post workout protein shake is so established that the debate has been more about whether to take high gi or low gi carbs, if waxy maize is better than dextrose. and so on. But this recent study shows that carbs may not be required in the first place.

Why carbs were needed in your workout protein shake?
Protein break down: Protein breakdown is increased after workouts. Carbs increase insulin levels and can blunt protein breakdown after your workouts. This is the major reason why carbs are added with protein shakes.
Protein Synthesis: Carbs can increase insulin levels and slightly increase protein synthesis.
Glycogen: Restore glycogen in the muscle. Unless you are doing a lot of high reps, glycogen is not really depleted with weight training.
What was the study design?
What were the results of the study?
Are there other studies to support?
30 gms vs 90 gms: Another recent study looked if 90 gms of carbs +amino acids can decrease protein breakdown compared to 30gms+amino acids after resistance training. But they didn’t find any significant difference between the groups.
Though study lacked a group with only protein to see if there is any difference if only protein was ingested, the results are consistent with this study.
Practical Applications
Related
How Much Protein Do You need After Your Workout?
Is Exercise or Cardio Exaggerated in Losing Weight?
Related Articles
Are Low Reps Ideal for Strength?
December 14 2010
Every now and then, you will articles saying bodybuilders should do low reps since that will help them increase their strength. And you will also see training programs for muscle which will have a mix of low and high reps to target both strength and muscle.

But are low reps ideal for strength?
Why is low rep considered ideal for strength?
Powerlifters: Powerlifters are the strongest blokes around, and their training involves a lot of low reps ( 1-6 reps).
Guidelines: According to text books and exercise guidelines, the repetition range for strength is 1-6 reps.
So what is the problem?
Types of strength: There are different types of strength: Maximal strength is the amount of weight you can lift for one repetition. And people are usually refferfing to maximal strength when they say just strength.
On the other hand, strength endurance is the maximum amount of weight you can lift multiple number of reps, say 15-20.
Specificity of strength: According to the theory of specificity, strength is very specific to the repetition range.
So if you want to increase your maximal strength, you do a lot of low reps (1-6). If you want to increase the weight you do for 10 reps, you do a lot of reps around 10 (8-12). If you want to increase your 20 reps, you do a lot of 20 reps ( 18-22).
Example: Consider 3 people A, B, and C with the same genetics, diet, body weight and motivation. A does a lot of bench press in the range of 1-6, B does a lot of bench press in the 8-12 range, and C does a lot in the 20-25 range. Who is stronger?
A is the strongest in 1-6 reps
B is the strongest in the 8-12 reps
C is the strongest in the 20-25 range.
Is there any evidence for this?
The above example was tested in a study. The first figure shows what happens when they were tested for maximal strength. As predicted, A was the strongest.
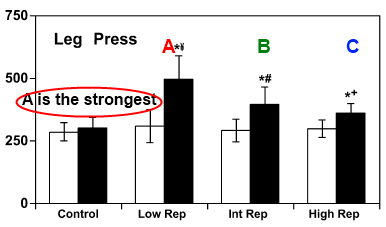
In the second figure, they were tested for strength endurance. And guess what, A was the weakest!
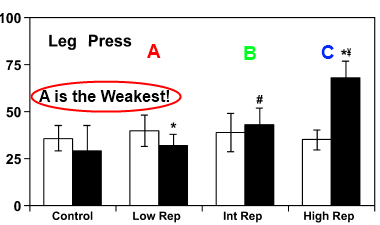
Practical Applications
Related Articles
How to Build and Stretch your Calf Muscle?
December 05 2010
You can emphasize the soleus or the gastroc with different exercise and stretches. Here we use the concept of active and passive insufficiency.
What are the different calf muscles?
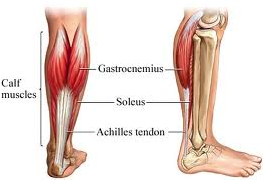
Gastrocnemius: Gastroc is the muscle which has two heads and is visible from outside as two diamond heads. Gatsroc has 2 functions: Bending the knee and raising your heel.
Soleus: Soleus lies beneath the gastroc and is not really visible. The soleus performs just one function of raising the heel as in calf raises.
How to build your soleus and gastroc muscles?

Seated Calf Raises: Seated calf raises target the soleus than the gastroc since gastroc is almost inactive during bent knee exercises.
The gatsroc is already used when the knee is bent and hence it cannot work to raise the heels. This is called the principle of active insufficiency.

Standing Calf Raises: On the other hand, standing calf raises emphasizes both the gastroc and soleus equally well.
How to stretch your soleus and gastroc muscle?
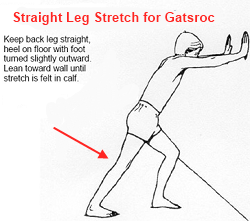
Straight Knee: Straight knee primarily stretches the gastroc.
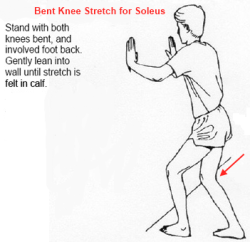
Bent Knee: Bent Knee stretches target more of the soleus since the gastroc muscle is contracted.
Practical Applications
Related
How To Make Your Ab Exercises More Effective
When You Should Change Your Exercises?
Related Articles
Can Vitamin C Prevent and Treat Common Cold?
November 28 2010
Should you take vitamin C to prevent and treat colds? Let’see what does this 2010 review add to the topic.

Why look at vitamin C?
What were the study highlights?
The study is a systematic review. Out of 55 studies, 36 met the inclusion criteria.
What were the vitamin C study results
Practical Applications
Related
Can Antioxidants Prevent Cancer?
Is Creatine Ethyl Ester Better than Creatine Monohydrate?
Related Articles
Evidence-Based Approach to Fitness/Sports Performance
November 21 2010
From what I have seen, most folks have very little understanding of an evidence-based approach. They think EBP is all about taking the results of a study and just blindly applying it. This is called research utilization and is clearly NOT evidence-based approach.
So what is the definition of evidence-based approach?
As the figure shows, evidence-based approach involves the integration of the best available evidence with the trainer’s/coach’s expertise and the client values, goals, and circumstances.
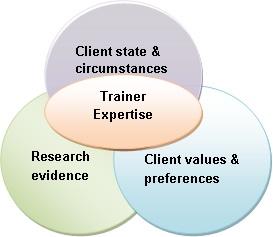
Best available evidence from research
The experience and expertise of the coach/trainer
client concerns, values, circumstances, & preferences
The above is just a very brief introduction to the topic of evidence based approach.
There is certainly more to it like hierarchy of evidence, grading of evidence, appraising the evidence and so forth, but this article is certainly a good place to start. Unfortunately, in the fitness/performance field the research evidence part is missing and the decision making is solely based on the trainer experience/expertise and client goals and preferences.
Let me know what you think of the article.
Related Articles

Can Eccentric Training Increase Muscle & Strength?
November 06 2010
The meta-analysis (2009) looked to see if eccentric training is superior to concentric training for strength & muscle mass.
Why eccentrics are different from concentrics?
Eccentrics involve active lengthening and concentrics involve active shortening of the muscle fibers
Characteristics of eccentric contractions
What were the study highlights?
What were the results of the meta-analysis?
Practical Applications
Related Articles
What is Wrong with Testimonials and Results?
October 20 2010
Every trainer and fitness website has a testimonial page with a lot of impressive before and after pictures. And everyone claims it’s all about results. But what is blatantly wrong with these testimonials and results?
And this is the typical strength coach and trainer’s classic line: “I get results and results are all that matters”. Do you?

What is missing in testimonial and results?
Negative results: Have you ever seen a testimonial page with people looking the same in before -after pictures? Or anyone writing about how the program or the supplement didn’t do anything good for them?
For example, the testimonial page shows 10 people who got great results with the diet/workout program. But here might be 9 more people for whom the diet/workout didn’t do anything and 2 more people where the program/diet actually made them worse. These people are never seen of the testimonial page. Do you think the diet/ program still works?
Drop Outs: There are folks who dropped out from a diet or workout program and you will never find their names on a testimonial page. These are the people who usually think the program and supplement didn’t work for them. In drug trials of fatal diseases, like cancer, they usually say “dead men say no tales”.
What about research?
Reporting Bias/Outcome bias: In research this type of under-reporting is called publication bias or/and outcome bias.
In research, you have to report negative results, adverse outcomes, and the study drop outs /attrition rate. The effectiveness of a treatment/supplement is identified by taking into account BOTH the positive and the negative results. If you do not report negative results, you are in violation of the standard code of scientific conduct & ethical behavior and may end up in some legal trouble.
Practical Application
Related Articles
Does Glucosamine Chondroitin Help knee and Joint Pain Due to Osteoarthritis?
October 09 2010
Glucosamine Chondroitin is the most popular supplement for joint pain. But does it really help?
What is osteoarthritis?
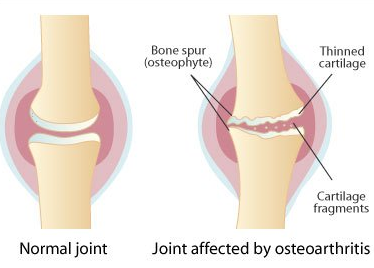
Why use Glucosamine & Chondroitin?
Why study again if it is already being used?
What were the major study points?
Trials compared chondroitin sulphate, glucosamine sulphate, glucosamine hydrochloride, or the combination of any two with placebo or head to head.Hence the name network meta-analysis.
Practical Applications?
Related Articles
The Top Natural Bodybuilders
October 03 2010
Like the Mr.Olympia, there is no single federation where all the natural bodybuilders compete.So it is hard to pick the best or the biggest natural bodybuilder.
In my opinion, these are the best natural bodybuilders (in no particular order) who have stood out in the recent years. Note that all these natural bodybuilders are currently competing. These are also some of the The biggest natural bodybuilders you will ever find.
Phillip Riccardo
Age: 39
Competition Weight: 180


Kiyoshi Moody
Age: 40
Competition Weight: 195-200


Doug Miller
Age: 33
Competition Weight: 186-192

Jim Cordova
Age: 31
Competition weight: 170-180


Jeff Rodriguez
Age: 27
Competition Weight: 180’s
Who do you think is the biggest natural bodybuilder?
And just to give you some perspective. Here is what drugs can do to you.
Jay Cutler
Mr. Olympia 2010 (Not Natural).
Age: 37
Competition Weight: 270!

Related Articles
The Top 5 Exercise Journals
September 26 2010
Most folks and even exercise science experts are unaware of how journals are rated and how these rating affect on the quality of the studies published .

Which are the top 5 exercise & sport journals?
1. Journal of Applied Physiology (3.73)
2. Medicine and Science in Sport & Exercise (3.70)
3. American Journal of Sports Medicine(3.60)
4. Exercise & Science Sports Reviews (3.62)
5. Sports Medicine (3.11)
The popular Journal of Strength & Conditioning Research is ranked 34 (1.457)! Their secondary journal Strength & conditioning Journal is ranked 64!
* These are 2009 ranking and subject of category is “sports science”
What are these journal rankings based on?
These ranking are based one the most popular bibliometric indicator called the Journal Impact Factor. The journal Impact Factor was first published in 1961.
What are the limitations?
There are number of limitations for this ranking system. Some of them are:
So why do people still rely on impact factor:
Impact Factor is extremely important in the research circles.
Usually getting an article published in Nature or Cell is a dream for most researchers. Some of the researchers (atleast the ones I worked with) doesn’t even bother reading articles published in low impact journals.
Practical application
Related Articles
Is Effort or Weight Lifted Important For Muscle Growth?
September 19 2010
Weight Lifted: Is defined as the amount of weight you can lift. This is usually denoted as 10 RM or 5 RM.(for ex, 5RM or 5 Repetition Maximum is the maximum amount of weight you can lift for 5 reps.)
Is weight lifted or effort Important for Muscle Growth?
Type 2 Fiber Recruitment: Type 2 fibers are the fibers which makes you big. They have greater growth potential and much stronger than Type 1 fibers. According to the size principle, the greater the effort, the greater the activation of Type 2 fibers. If the weight is heavy ( less than 6 reps), all fibers are recruited from the first rep. For moderate weights (greater than 6 reps), it is the effort in those last few reps that determine Typ2 fiber recruitment . Protein Synthesis Studies: In line with the Type 2 fiber recruitment, recent studies have shown that moderate weights taken close to fatigue can stimulate protein synthesis to a similar extent as heavier weights. Occlusion studies clearly shows light weights with greater effort can cause similar muscle growth to using heavy weights. Anecdotal Evidences: It is common to hear natural bodybuilders say it is the intensity (or effort) that matters not the repetition range and the program. The same goes with power lifters. Most people think it is not the program but the crazy training intensity at their gym is what makes Westside lifters among the best power lifters in the world.Practical Recommendation
Related Articles
Power Plate: Do Vibration Plates Work?
August 21 2010
Power plates seems to be the latest trend in the fitness indusrty. And there are number of studies done on these vibrating exercising machines. Let’s take a look at what the science say about the power plate.
What is a Power Plate?

Power Plate, one brand of vibration plate, as the name implies uses whole-body vibrations while you perform exercises on the plate.
What are the power plate performance & health claims?
The power plate company claims that power plate helps:
Their most marketed claim is the increase in strength and power and how it is used by elite level athletes in the NBA, NFL, and pro golf players. Here is a qoute from their website:
“For serious athletes, workouts on the Power Plate® machines enhance the results of conventional training and explosive strength training, as well as serve athletes and trainers alike to speed recovery and regeneration times. Because of the extensive academic and independent scientific research, professional sports teams throughout the world use Power Plate® machines as part of their strength and conditioning programs.”
So does power plate help in increasing strength and power?
There are number of long term studies which looked at strength, power and speed changes with vibration training. The power plate website quotes number of studies which show significant increase in strength and power. But almost all of these had serious methodological issues as shown below:
Looking at all the studies, we can conclude that:
Can vibration training be harmful?
Practical Recommendations
Related Articles
CPR: Just Chest Compressions To Save Lives?
August 15 2010
Cardiopulmonary resuscitation (CPR) is a lifesaving technique that involves a combination of rescue breathing (mouth to mouth) and chest compressions delivered to victims in cardiac arrest.

In my opinion, this is probably the most useful skill you will ever learn in your life.
Why is CPR important?
What are the different methods of CPR?
Till date, besides animal studies and a few small studies, there has been no large human studies comparing the effectiveness of these 2 methods on survival.
What does the recent studies suggest?
Two recent large studies (1900 and 1300 hundred people) published in the top clinical journal - New England Journal of Clinical Medicine - suggest that continuous chest compression CPR by bystanders is as effective for survival as the traditional CPR of rescue breaths.
Why is chest compression CPR better?
Should we stop doing rescue breaths?

How do I do Chest compression CPR?
This video only takes 2 minutes.
Related Articles
Which Is The Best Weight-Loss Diet?
August 09 2010
The best weight loss diet is still intensely debated and there has been very few well conducted studies which looked at this issue. Is a high protein diet better, or high carb or a high fat diet the best weight loss diet?

A recent study looked to find out which is the best weight loss diet and received a lot of good attention.
What were the strengths of the best weight loss diet study?
What was the design of the best weight loss diet study?
Eight hundred and eleven participants were randomly assigned to four different diets:
All of the diets had an average calorie deficit of 750 calories from the patients’ aggregate baseline caloric intake. Participants followed the diets for two years, during which time they were also expected to engage in 90 minutes of moderate exercise each week, keep a daily food diary, fill out a Web-based tool that monitored how closely their intake adhered to their assigned diet, and attend group and individual sessions to promote adherence
What were the results of the best weight loss diet study?
All the diets were equally successful in promoting moderate weight loss and maintaining this loss for over 2 years. Weight loss averaged 3-4 years after 2 years.
Practical Recommendations
Related Articles
Is Single Set or Multiple Sets Better To Build Muscle?
July 31 2010
The question of single set or multiple sets for building muscle has been long standing. A recent study has shed some new insight into this “number sets for muscle” debate.
Why one set to build muscle?
Why multiple sets to build muscle?
But what do the studies say?
What was the design of the study?
The recent study looked at one set and 3 sets on muscle protein synthesis.
What were the results of the study?
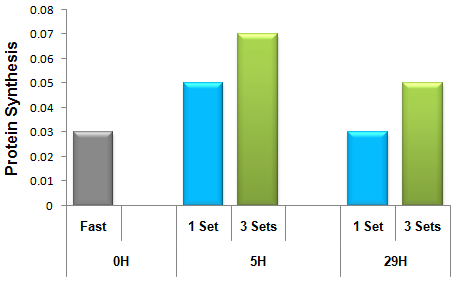
What about long term studies on sets and muscle?
Can this acute results in protein synthesis translate as muscular changes in the long term? Yes, indeed.
Practical Recommendations
Related articles
Related Articles
The Best Stretch For Your Shoulders
July 25 2010
There are number of shoulder stretching exercises. But which is the most important and why?
Why stretch the shoulder posterior capsule?
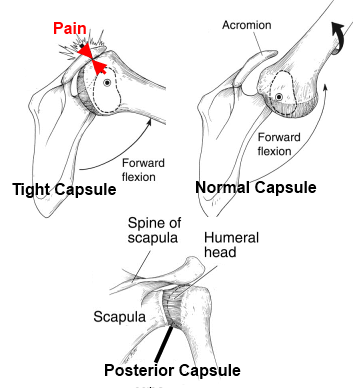
Figure: The figure shows how a tight posterior capsule can cause impingement and shoulder pain when you raise your arm.
What are the stretches for the posterior capsusle?
The two most common stretches for posterior capsule are:
1. Sleeper stretch
2. Cross body stretch.


So which is the best shoulder stretch?
Of the two, a recent study showed that the cross body stretch to be more effective for posterior capsule and increasing IR range of motion compared to sleeper stretch
Practical Application
Related Articles
The Best Scapular Muscle Exercises to Prevent & Treat Shoulder Pain
July 17 2010
There are number of exercises to optimize scapular muscles to prevent and treat shoulder pain. But which are the best scapular muscle exercises?
What are scapular muscles?
Scapular muscles are muscles that connect to the scapula and give both stability and mobility to the scapula, which is unique among other joints . The major scapular muscles are shown in the below picture.
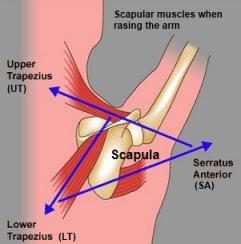
Why scapular muscles are important in shoulder pain?
Scapulothoracic Rythm: The scapula has to move in a well-coordinated manner as shown to bring about arm movements. Any change in the function of scapula muscles can affect the normal functioning of the shoulders.
Correlation: Very recently, number of studies have shown abnormalities in scapular position and motion to be correlated with shoulder pain caused by impingement symptoms, rotator cuff dysfunction, and instability.
Shoulder Rehab protocols: All shoulder rehab protocols now emphasize the importance of scapular muscle training as a component of shoulder rehabilitation.
Which scapular muscles are important ?
Most researchers attribute scapular dysfunction to scapular muscular imbalance rather than absolute strength deficits of the scapular muscles.
In particular,excess activation of the upper trapezius (UT), combined with lower activation of the lower trapezius (LT) and the serratus anterior (SA), has been proposed as contributing to abnormal scapular motion (muscles shown in pic).
Hence the best scapular exercises are those which have high activity of LT & MT and low activity of UT.
So which are the best scapular muscle exercises?
If you have any questions about these scapular exercises, just ask in the comment section.
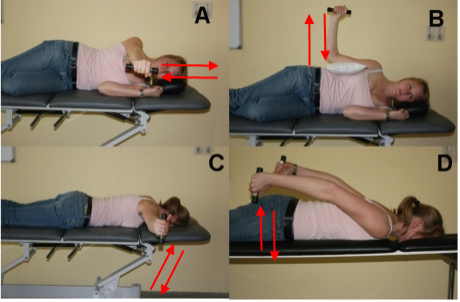
Related Articles
Why Some Grow Muscle Easily While Some Don’t?
June 01 2010
The study shows why some folks grow like a weed while other struggle.
The study recruited 66 subjects.The training included 3 sets of squats, Leg Press and Leg Extensions 3 days/week for 16 weeks.
What were the results?
Based on the muscle fiber size, the participants were divided into three groups independent of age or sex ( using new method called cluster analysis):
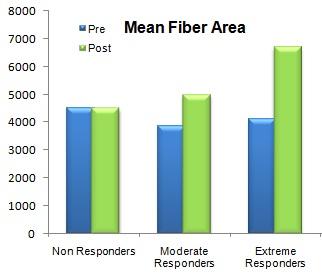
Extreme Responders: 58% increase in muscle fiber size
Moderate Responders: 26% increase in muscle fiber size
Non Responders: 0% increase in muscle fiber size.
What are satellite cells and muscle nuclei?
Before you can understand the results of the study, you need to be familiar with some terms. I will keep it simple and short, promise.
Unlike other cells in the body, muscle cells (or muscle fibers) are multinucleated. Considering how a muscle cell is way larger and complex than the rest of the cells in the body, it makes a lot of sense to have more than one nuclei to control the complex tasks in the muscle.
For instance, if your favorite restaurant was a muscle and the cooks the nuclei, it’s pretty safe to say that the number of cooks sets the limit to the size of the restaurant. Similarly (or somewhat), the size of your muscle is ultimately limited by the number of nuclei you have in your muscle.
Simply put, you cannot grow bigger muscles without additional nuclei to take care of the extra muscle.
So where do we get these nuclei from?
Figure: A muscle fiber with nuclei shown in blue and satellite cell shown in red.
These muscle nuclei sprouts from specialized cells around the muscle called satellite cells. So any increase in satellite cells means some of these cells could be “blossoming” into new nuclei.
So how did the extreme responders grow muscle easily?
NOTE: It is interesting to note that 1/4(non-responders) of the subjects experienced no growth. The authors speculate that this might be because of a lack of greater recovery period between workouts and/ or additional weeks of training. Studies with 2 days/week has shown better results in older adults.
Practical Recommendations
Related Articles
How Graphs Can Fool You
May 18 2010
You can be easily tricked into believing things if you don’t read the actual data and just glance at the graphs. Below are some of the ways how graphs tend to fool you.
Distortion of Scale
Here the units of the graph are distorted to make the differences between groups to look much larger than what it is. The second graph shows the more accurate representation. The difference in strength in Group A is made to appear triple that of Group B though it is only a 10 lb difference.
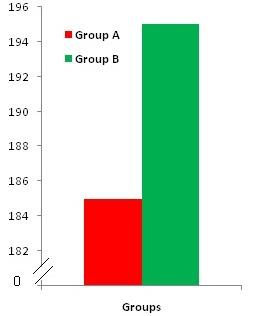
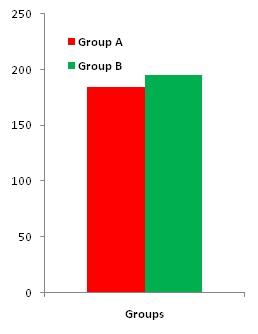
The score above 70 represents clinical depression. The decline of depression scores over 72 months is only 3.5 scale points but is made to look significant by distorting the units. The second graph is shown in the correct scale.
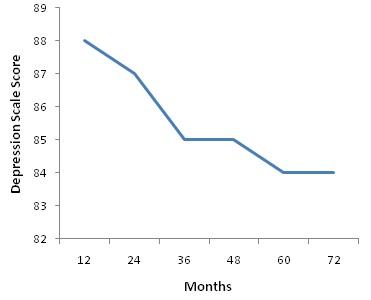
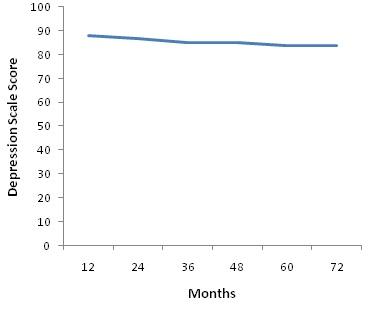
Distortion of Meaning
The graph shows the difference in tempertaure to be trivial though 98.6 is normal and 102 is significantly elevated. The second graph shows a meaningful representation considering it shows the percentage of people in each group who exceeds the normal temperature of 98.6.
Linearity Distortions
In longitudinal studies, it is usually customary to connect the pre and post test values with a straight line which can distort the true picture.
The graphs shows the changes in weekly income. The first graph shows measure taken only at the start and end dates which misleadingly suggests a steady rise in income. The bottom graph provides the monthly data and the true picture.
Related Articles
Connect with us
![]() Add us on Facebook
Add us on Facebook
![]() Get tweets
Get tweets
![]() Subscribe to RSS feeds
Subscribe to RSS feeds
![]() Get email updates
Get email updates
About the site
Exercise Biology stands far part from other fitness sites by taking an evidence-based approach to common man's health, fitness, & nutrition. Thanks for visiting Exercise Biology.About me

© 2008 - 2025 | Exercise Biology. All rights reserved.